In recent blogs we have reviewed the correct techniques for measuring the size of the left ventricle and the aorta. This week we will review the correct way to measure the left atrium. The updated standards on chamber quantification, released last year by the American Society of Echocardiography, provided new information and guidelines on correct measurement of the left atrium. There was a huge change to the reference range of the left atrial size.
HUGE!
You know you’re an echo geek when you hear the word “HUGE” and the first thing you think of is the changes to the reference range for left atrial size! The changes to the reference range for the left atrial volume were so significant (huge, in fact!) that patients once diagnosed as having severe LA enlargement now fall under moderate and even mild left atrial enlargement!

According to the 2005 guidelines patients with a LA index volume of 41 would have been diagnosed with severe left atrial enlargement. With the latest updates this same patient would now only be diagnosed with MILD LA enlargement!
WHY THE HUGE CHANGE TO THE REFERENCE RANGES?
The short version is that the previous data was wrong! Dr. Lang (the co-chair of the writing committee for both the 2005 and 2015 guidelines) explained at the 2015 Scientific Sessions in Boston that when they were writing the 2005 Guidelines the data for the LA reference range was gathered from only 2 published studies with a small number of subjects. The data used for the 2015 Guidelines, on the other hand, incorporated an additional 8 studies plus 5 data bases that totaled over 2500 subjects. The results were that the LA is a lot larger than we originally understood it to be.
HOW TO CORRECTLY MEASURE THE LEFT ATRIUM
For decades the most commonly used method for measuring the left atrium has been the M-Mode or 2D measurement from the parasternal long axis view measuring anteroposterior (AP) dimension. The new guideline state that the “AP linear dimension should not be used as the sole measure of the LA size”. The recommendation to assess the LA size is to measure the volume of the LA. Why?
I believe that once sonographers truly grasp why we should change the way we do something that we will embrace the change. Let’s review why measuring the LA in only one plane would sometimes cause an inaccurate measurement.

By only measuring the left atrium in one dimension (The AP parasternal long axis view) we are assuming that when the left atrium enlarges that it expands equally in all dimensions. We think that we have accurately depicted the size of the LA. But what happens during LA remodeling when the atrium does not enlarge equally? Can you measure something in just one plane and accurately report on its size?
Think of this in a real world setting. Meet Peter and Paul. They have the same dimension of height. They are both the same height but are they the same size??? When we measure the left atrium and report only on the AP measurement from the PLAX view it would be the same as reporting that Peter and Paul are the same size! Although it’s technically a true statement we would not be reporting accurately about their size. When we rely solely on the Parasternal long axis AP measurement of the left atrium, we are not always reporting accurately about the size of the left atrium.
BUT I STILL WANT TO MEASURE THE ATRIUM IN PARASTERNAL LONG!!
Don’t worry you are not alone. As mentioned, for decades the most commonly used method for measuring the LA has been from the PLAX. Now that the LA volume is measured, technically you do not need to measure the LA in PLAX anymore. However, due to the common clinical use of this measurement the new guidelines provide updated recommendations on how to accurately measure the LA in PLAX. I will quickly review the correct techniques for measuring the LA in the PLAX view but promise me you will never use this as the sole measurement for the LA!
4 TIPS FOR THE CORRECT TECHNIQUE TO MEASURE THE LA IN PLAX:
- Preferred method is transthoracic echo not TEE
- The entire LA does not fit in the sector screen during a TEE
- Measure in 2D not M-Mode
- ASE recommends 2D measurements as it allows for perpendicular alignment to the plane of the LA
- Measure at end-systole when the atrium is at its largest
- Pay attention to the size of the LA not the ECG
- Measure at the level of the midpoint of the sinus of Valsalva
- This location correlates with the position of the cursor with M-Mode. Original values for the LA were obtained from M-Mode.
TEST YOUR KNOWLEDGE:
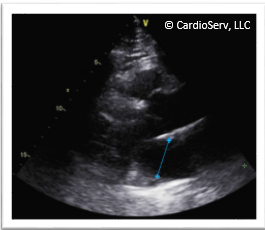
Here is an image that came across my desk. Why is this LA measured incorrectly?
A. Left atrium should be measured in M-Mode
B. Measurement is not perpendicular to the plane of the LA
C. Artifacts are affecting the correct measurement
D. Image is not measured in end systole
The correct answer is B – the measurement is not perpendicular
to the plane of the LA
Although the anterior cursor is close to the mid-point of the sinus of Valsalva the posterior cursor was placed too inferiorly, creating a plane that is NOT perpendicular to the plane of the LA. The corrected image is perpendicular to the plane of the LA.
What about the artifact? As you can see from the corrected image, once the correct cursor placement is made perpendicular to the LA, the measurement is no longer affected by the slice thickness artifact seen in the image.
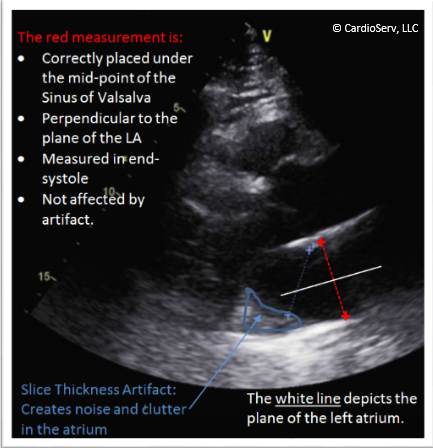
SLICE THICKNESS ARTIFACTS:
This artifact is often seen in the PLAX view creating noise and clutter in the LA behind the posterior MV annulus. I often see sonographers’ under-measure the left atrium due to this artifact. Without getting too geeky this kind of artifact is mostly a technical limitation of ultrasound versus an issue with correct techniques as it is due to the bright reflector underneath the atrium (beyond the focal zone) that affects the anechoic space above it. Some tricks you can try to help resolve this include moving the focus up or down and repositioning the patient. The main thing is just to be aware of this common artifact when placing your cursor and avoid underestimating the size of the LA.
LA VOLUME
So now you understand why the linear measurement in the PLAX view is not enough to accurately report on the size of the LA volume, it’s time to learn the correct techniques for measuring the left atrial volume. Let’s review the reference ranges again. Notice the LA volume is reported as Volume/BSA. What does that mean?

The research data found that the LA size is actually dependent on gender. However the gender differences in LA size can be accounted for when adjusted to body size. Therefore the recommendation is to index the volume to the patients’ BSA (body surface area). This just means you have to enter the patients’ height and weight into the ultrasound system so that it has the necessary information to calculate your LA volume as an indexed LA volume/BSA.
BI-PLANE DISK SUMMATION
The updated ASE Guidelines now recommends using the biplane disk summation technique as the preferred method for measuring the LA volume. (In 2005 both the biplane disk and the area-length method were recommended). Calculating the LA volume using the disk summation algorithm is considered to be the most accurate method for calculating the LA volume as it does not make any geometric assumptions regarding the shape of the LA. This allows for accurate measurement of asymmetric remodeling of the left atrium.
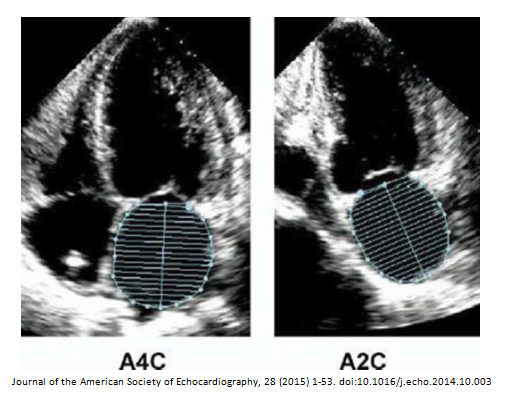
The example of correct technique for measuring the LA volume provided in the guidelines show:
- Left atrium traced in END-SYSTOLE in both the apical 4 and 2 chamber views
- Trace from the level of the mitral valve annulus
- The left atriums are not foreshortened
- The length is perpendicular to the annular plane
- Make sure you check the settings on your ultrasound system default to the biplane disk summation and not the area-length method
- Remember to enter the patients’ height and weight so the software can calculate the indexed Volume/BSA
Sounds simple enough, right? Unfortunately, after spending the day looking for the perfect example of correct LA volume technique I came up empty. Instead I found case after case with similar mistakes and errors.
PITFALLS TO AVOID
As I mentioned in a previous blog, sonographers are often asked to perform new measurements yet provided with very little information on correct techniques. I have narrowed down the most common mistakes that I see to provide you with examples of pitfalls to avoid:
4 STEPS TO MASTERING THE CORRECT WAY TO MEASURE THE LA VOLUME
Although I found more incorrectly measured LA volumes than I did correctly measured LA volumes the good news is that you can be a LA Volume Guru with just 4 simple tricks! If you implement these strategies you will be amazed at the improvement you will notice immediately, they will be HUGE!
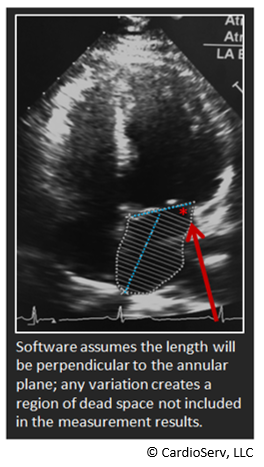
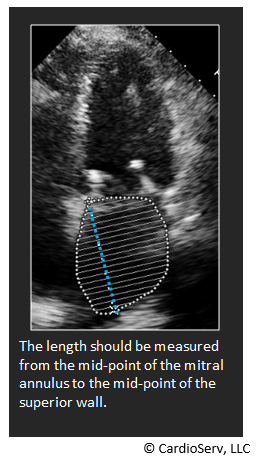
- Correct length measurement
- The length should be measured from the mid-point of the mitral annulus to the mid-point of the superior wall
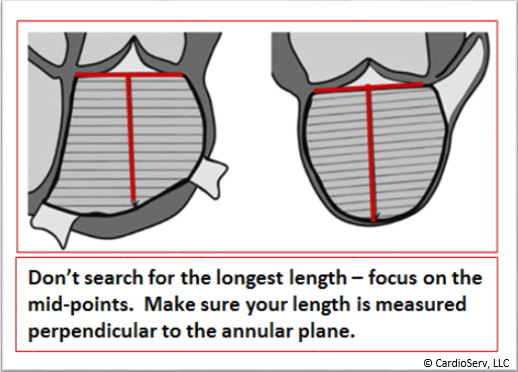
- Don’t search for the longest length but rather focus on the midpoints
- Make sure the length is perpendicular to the annular plane as the software that calculates the volume assumes this perpendicular relationship – any deviation from this creates a region of dead space
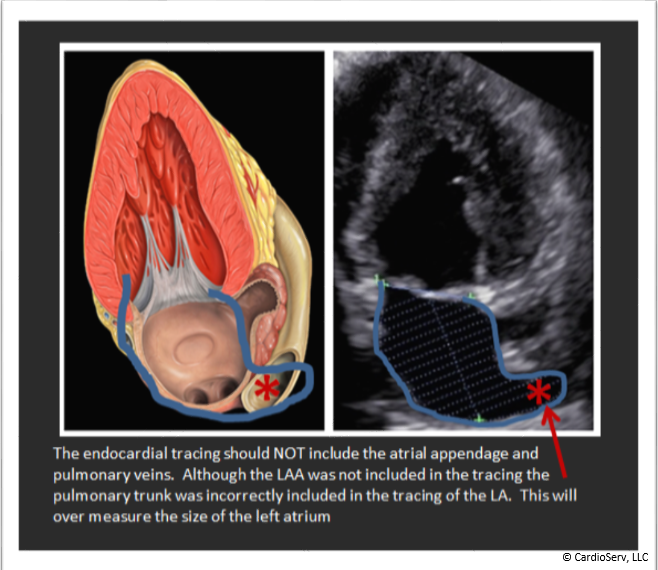
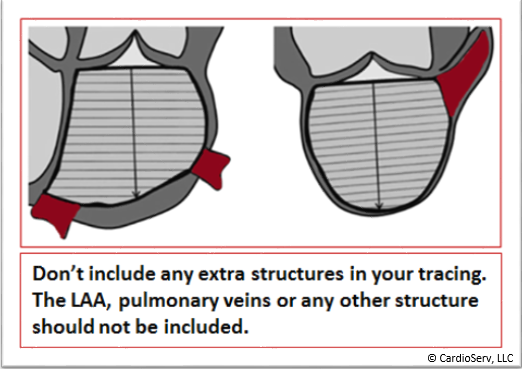
- Don’t include extra structures
- Do NOT include the LAA when measuring the LA
- Do not include any other extra structures including pulmonary veins or the pulmonary trunk
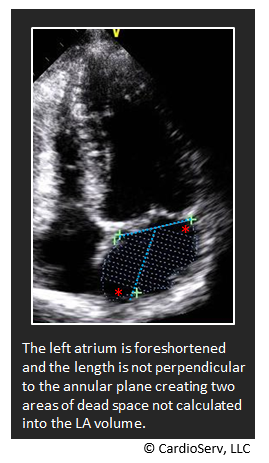
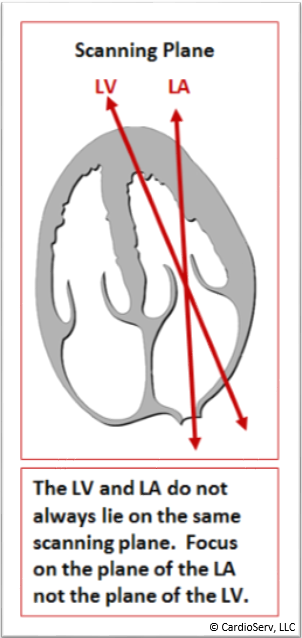
- Avoid foreshortening of the LA
- Do not focus on the LV plane but rather focus on the plane of the left atrium
- Pay attention to open up the left atrium to its fullest size in both the 4C and 2C views
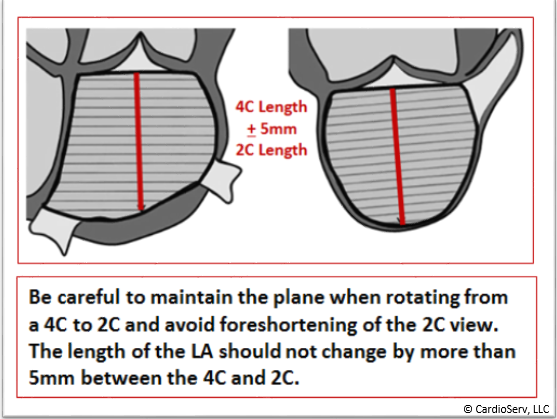
- Maintain the plane when rotating to a 2C view
- The length of the LA should never change by more than 5mm between the 4C and 2C views
- If the length difference is greater than 5mm, repeat both your 4C and 2C views to ensure accuracy
- It may help to obtain these 2 views sequentially within your scanning protocol
HUGE IMPROVEMENT WHEN ASSESSING THE LA!
My goal in writing these blogs is that you take away one or two points that will help you to improve the way you perform echocardiography within your lab and more importantly why we should implement these changes into our labs. This week I hope to have a HUGE impact on the way you evaluate the left atrium. Here is the summary of this weeks lesson:
- Significant changes to the reference range of size and severity of the LA size – post these in your lab for the physicians and change your normal values on your reporting templates
- Correct technique for the 2D parasternal long AP linear measurement of the LA – 2D, perpendicular to the plane, mid-point of the Sinus of Valsalva.
- The AP linear dimension should not be used as the sole measure of the LA size
- The LA size should be reported as an indexed LA Volume/BSA and measured using the bi-plane disk summation technique.
- Implement the 4 steps to mastering the correct way to measure LA volume
- Correct length measurement – perpendicular, mid-point to mid-point
- Don’t include extra structures – avoid LAA, pulmonary veins, etc
- Avoid foreshortening of the LA – Focus on the LA plane not the LV plane
- Maintain the plane when rotating – the 4C and 2C length should never change more than 5mm
CardioServ is an accreditation consulting firm specializing in full service accreditation in diagnostic imaging. Sign up for our newsletter and follow us on Facebook to get the most up to date news on cardiovascular imaging!