Before jumping into assessing the RV with the Fractional Area Change method, lets recap the past couple weeks. Last week, we talked about two methods for quantifying the function of the RV (TAPSE & S’ Wave). We selected these methods to explain first due to ease, reproducibility and established prognostic value. As some of our readers pointed out and as we discussed the TAPSE and S’ Wave methods do have limitations though. The 3 main limitations are:
- Angle dependency
- Load dependency
- Does not fully represent RV global function and therefore may over or underestimate global RV function
This week, we are going to discuss another method for evaluating the right ventricular function called fractional area change (FAC) which provides a better estimate of global RV function. As with most quantitative methods there are advantages and limitations. We will review the limitations of FAC along with the advantages.
This week you will learn:
- What is Fractional Area Change (FAC)
- How to perform FAC (fractional area change) to assess RV Global function
- Reference range of FAC
- Advantages
- Limitations
FAC: FRACTIONAL AREA CHANGE
1. WHAT IS FRACTIONAL AREA CHANGE?
Fractional area change (FAC) is a measurement that provides an estimate of the global RV systolic function. Remember this is a formula to calculate the % of area change within the RV between diastole and systole. The value provided is a percentage but please do not confuse this with the ejection fraction %. A normal value for the FAC is 35% or higher.
- Based upon area change – the value will be less than the calculated EF value
- Established prognostic value
- Reflects both longitudinal and radial components of RV contraction
- Correlates with RV EF by CMR
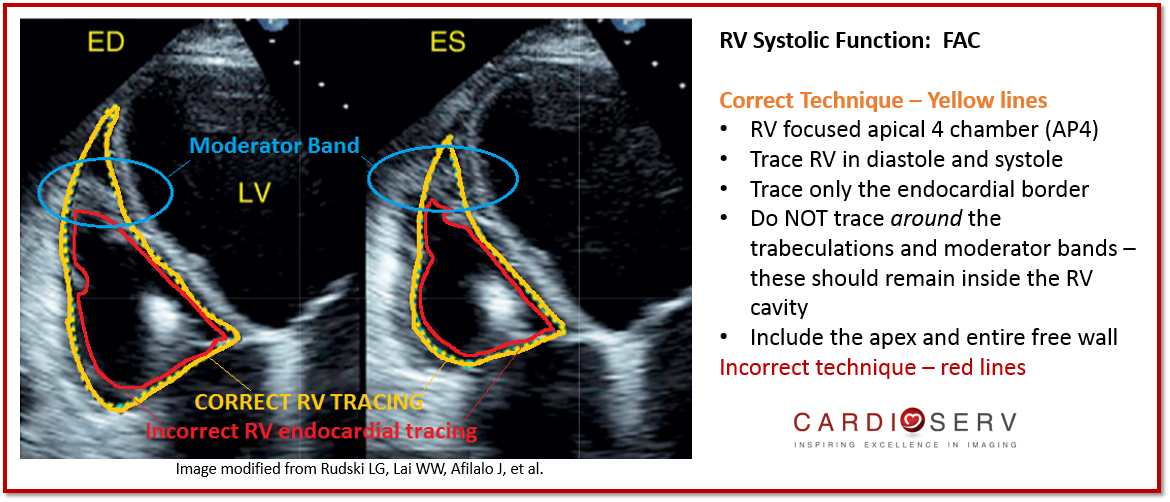
2. HOW TO CORRECTLY PERFORM FAC
- RV Focused apical 4 view (refer to prior blog on how to obtain this view!)
- Ensure entire RV is contained in imaging sector during both systole & diastole
- Trace RV area in diastole and systole (cm²)
- Be sure to include trabeculae & apex within cavity
Pitfalls to Avoid When Measuring FAC
- Avoid foreshortening of the RV
- Be sure to include the entire apex and free wall
- Trace the endocardial border – yellow line below
- Do not trace the borders of the moderator band and trabeculae ONLY trace the RV endocardial border
- Don’t measure what you don’t see! Remember there are others methods to evaluating RV Function you can use! (TAPSE or S’ Wave)

3. REFERENCE VALUES
Formula:
End diastolic area of the RV – End systolic area of the RV / End diastolic area of RV
This is a quick and easy calculation so don’t be afraid to use your calculator if your machine does not have a measurement package for this measurement!

Reference Range:
Remember this is the percentage of area change not the RV ejection fraction. Normal FAC values are greater than 35%. Anything below 35% is abnormal.

4. ADVANTAGES OF FAC FOR RV SYSTOLIC FUNCTION
- Established prognostic value
- RV FAC is found to be an independent predictor of:
- Heart Failure
- Sudden Death
- Stroke
- Mortality in patients after pulmonary embolectomy
- Longitudinal and radial components of RV contraction
- Correlates with CMR
5. LIMITATIONS OF FAC
- Neglects contribution of RVOT to overall RV function
- Limited inter-observer reproducibility
SUMMARY
FAC is listed by ASE as one of the quantification methods we’re able to use for evaluating RV function. It is a great representation of the estimated RV global systolic function. We’ve now discussed three different methods to use for quantifying RV function (TAPSE, S’ Wave and FAC). Next week, we will review a 4th method for evaluating RV function, RIMP! Thank you for your comments! Keep them coming as we all continue improving how we quantify the size and function of the right heart with echocardiography.
Recent Right Heart Blogs:
- 8 Things to Know About the Estimation of RAP
- Introduction to Right Heart Assessment
- 7 Tips to Implementing to Implementing RV Size Quantification
- 10 Tips to Correct RA Size Quantification
- 8 Tips to Correct RV Function Assessment with TAPSE and S’ Wave
WANT A CME FOR READING THIS BLOG? CLICK BELOW TO ACCESS CARDIOSERV’S ONLINE CME PLATFORM OFFERING CAT. 1 AMA CMES!


Judith Buckland, MBA, RDCS, FASE, President
References
Lang, R. M., MD, Badano, L. P., MD, & Mor-Avi, V., PhD. (2015). Recommendations for Cardiac Chamber Quantification by Echocardiography in Adults: An Update from the American Society of Echocardiography and the European Association of Cardiovascular Imaging. JASE, 28(1), 1-53. Retrieved March 1, 2017, from http://asecho.org/wordpress/wp-content/uploads/2015/01/ChamberQuantification2015.pdf
Rudski LG, Lai WW, Afilalo J, Hua L, Handschumacher MD, Chandrasekaran K, et al. Guidelines for the echocardiographic assessment of the right heart in adults: a report from the American Society of Echocardiography endorsed by the European Association of Echocardiography, a registered branch of the European Society of Cardiology, and the Canadian Society of Echocardiography. J Am Soc Echocardiogr 2010;23:685-713.
Kossaify, Antoine. “Echocardiographic Assessment Of The Right Ventricle, From The Conventional Approach To Speckle Tracking And Three-Dimensional Imaging, And Insights Into The &Quot;Right Way&Quot; To Explore The Forgotten Chamber”. N.p., 2017. Print.
Guazzi, M. et al. “Tricuspid Annular Plane Systolic Excursion And Pulmonary Arterial Systolic Pressure Relationship In Heart Failure: An Index Of Right Ventricular Contractile Function And Prognosis”. N.p., 2017. Print.