As technology advances and we are encouraged to implement additional measurements into our routine scanning exams, it’s good to take a step back and refresh on proper techniques! Our goal for this blog is to have a better understanding of proper technique for measuring left ventricle (LV) volumes!
In the ASE 2015 Chamber Quantification Guidelines, the recommended method for obtaining LV volumes is via bi-plane method of disk summation, aka: Simpson’s Bi-plane.
The standards clearly state that obtaining LV volumes via linear 2D measurements (Teichholz method) is NOT the recommended method.
WHAT IS THE BI-PLANE METHOD OF DISK SUMMATION?
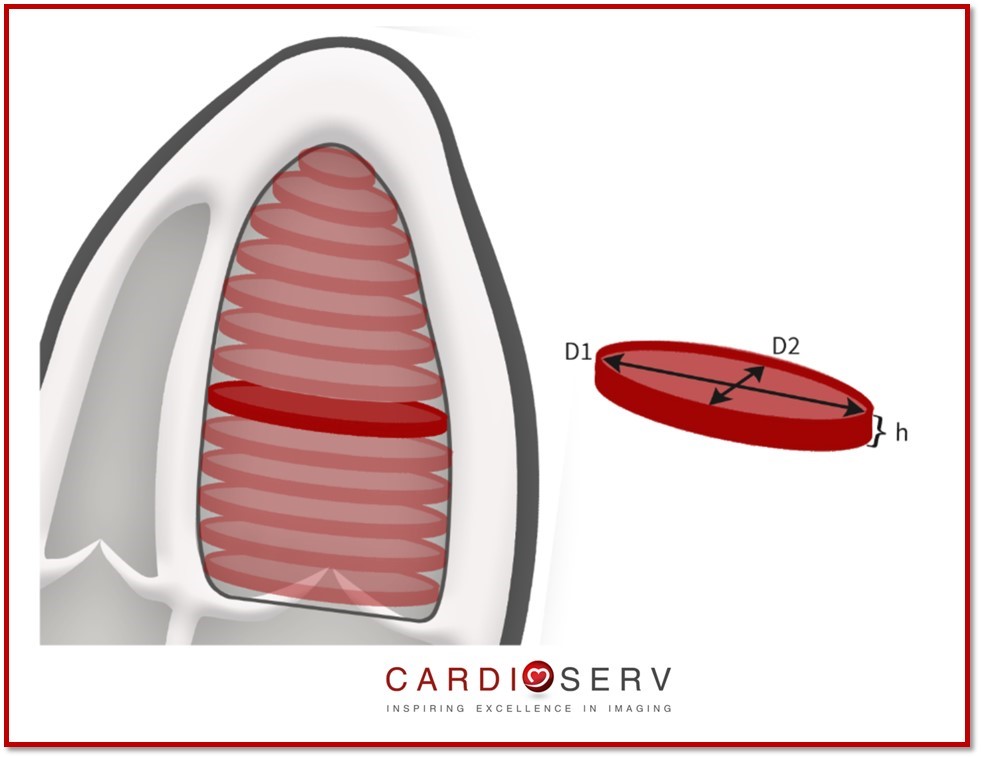
Biplane method of disk summation is a process of dividing the LV cavity into multiple disks (cylinders) of equal height. The length of the LV will determine the number of disks within the cavity. The volue (V) of each disk (n) is calculated using the length (D1) and width (D2). The height of each disk is calculated from the total length of the left ventricle divided by the amount of disks within the cavity (= L/n)
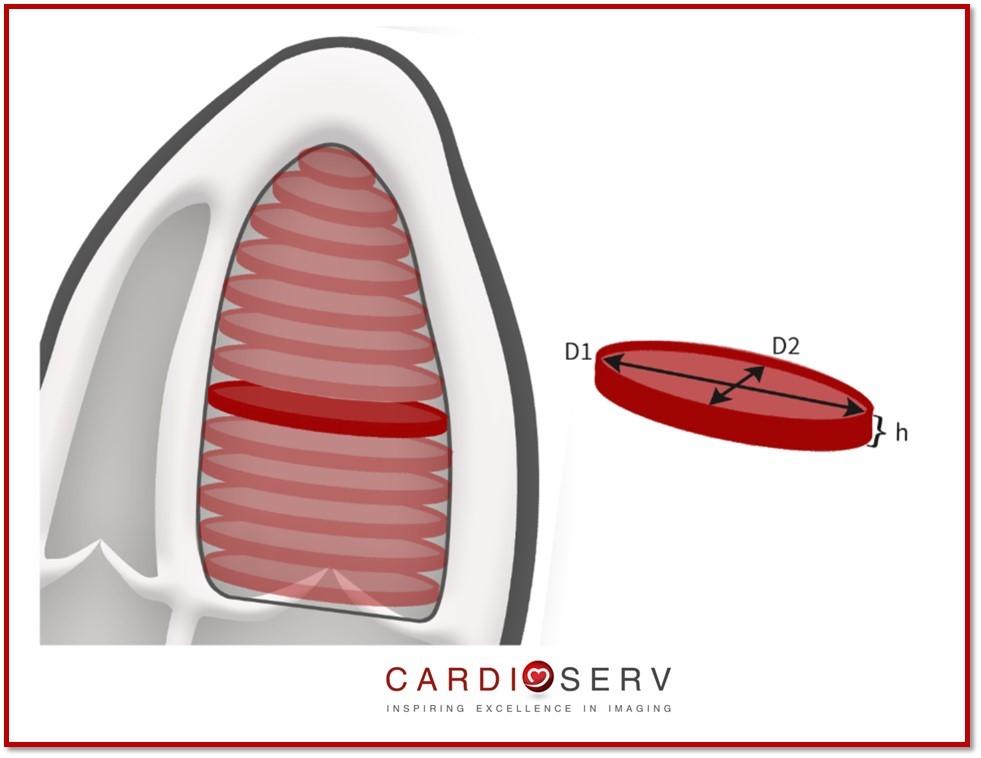

The volume of each disk will be calculated and formulated into the calculation package within our ultrasound machines to provide us with the end-diastolic and end-systolic volume of the left ventricle.
Advantages:
- Corrects for shape disortions
- Less geometrical assumptions
Disadvantages:
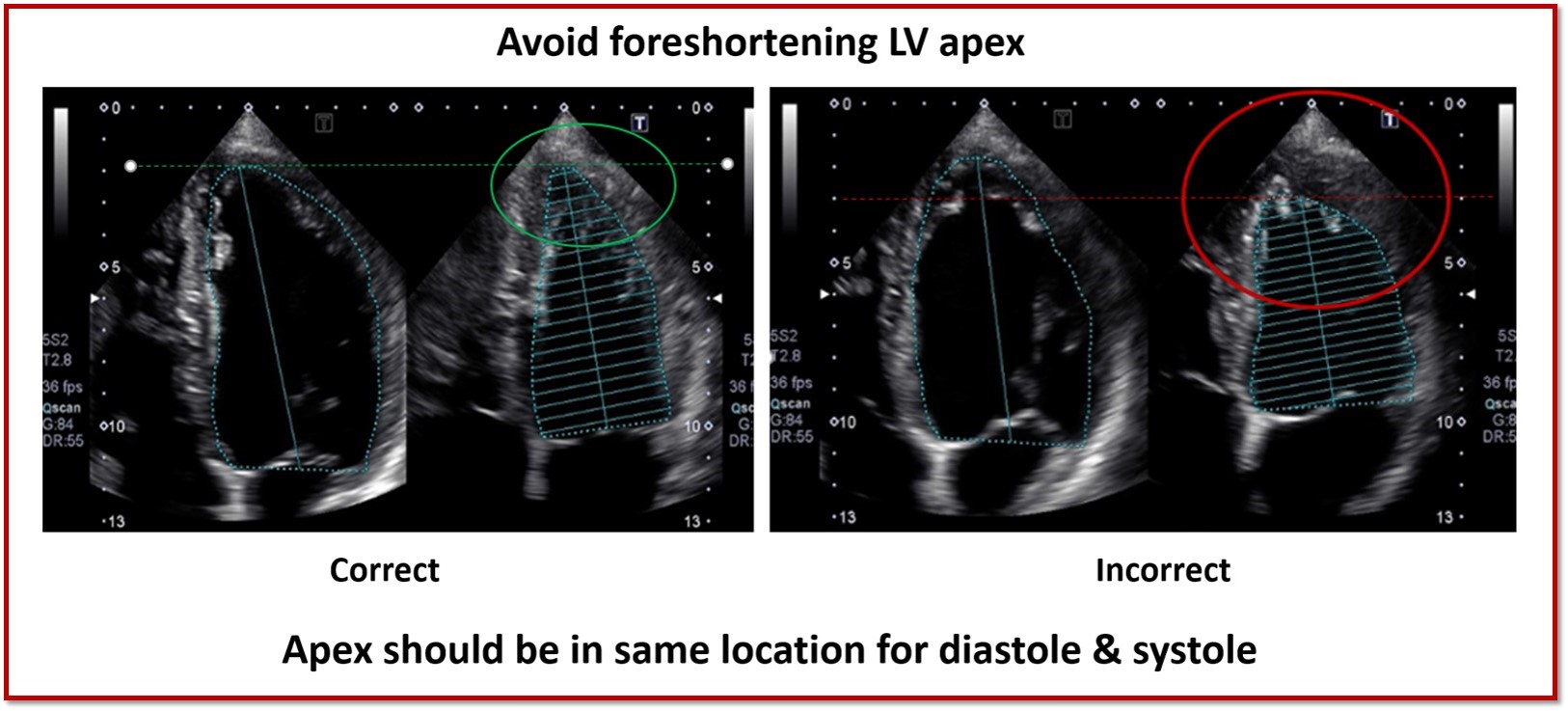
- Apex frequently foreshortened
- Endocardial dropout
- Not valid with LV shape distortions
HOW DO WE PERFORM BI-PLANE MEASUREMENT?
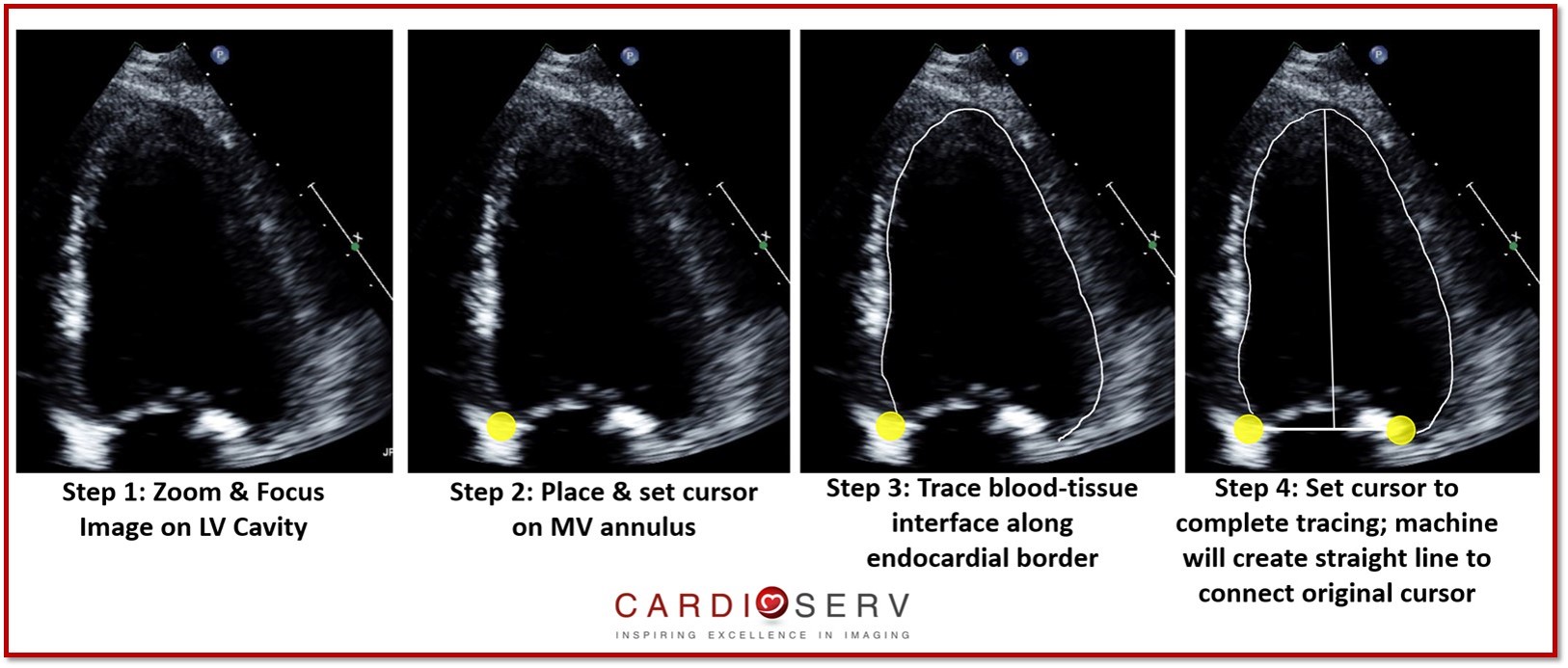
Bi-plane measurement is obtained by tracing the blood-tissue interface of the endocardial border within the LV cavity. The tracing is connect with a straight line at the mitral valve level, from the lateral to medial annulus points. The height of the cavity is taken from the middle point of straight line across mitral valve annulus to most distal point of LV apex.
We perform bi-plane measurement routinely in both apical 4 (AP4) and apical 2 (AP2) windows at end-diastole and end-systole.
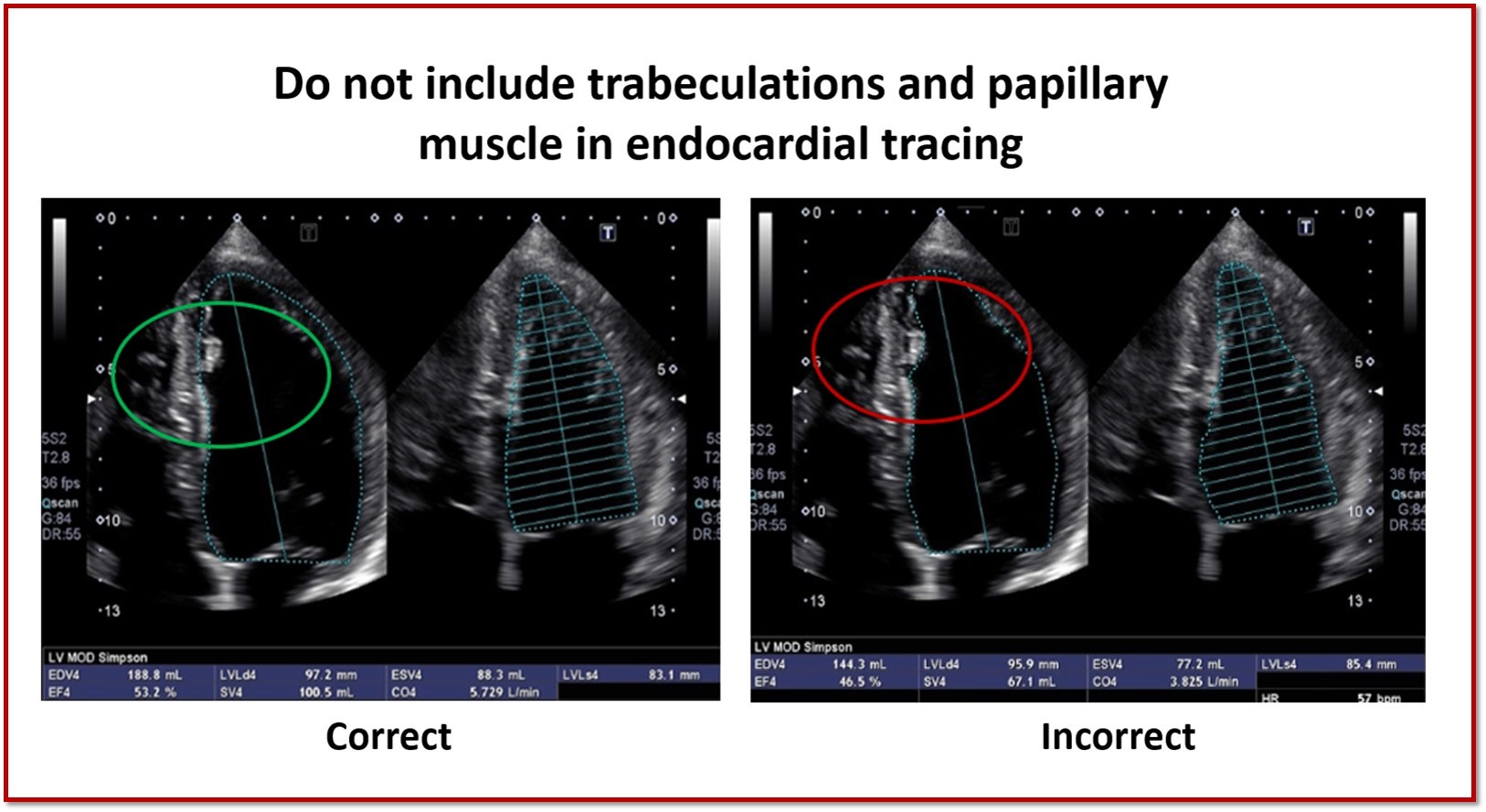
PITFALLS TO AVOID
- Do not include papillary muscle or trabeculations in endocardial tracing
- Avoid foreshortening
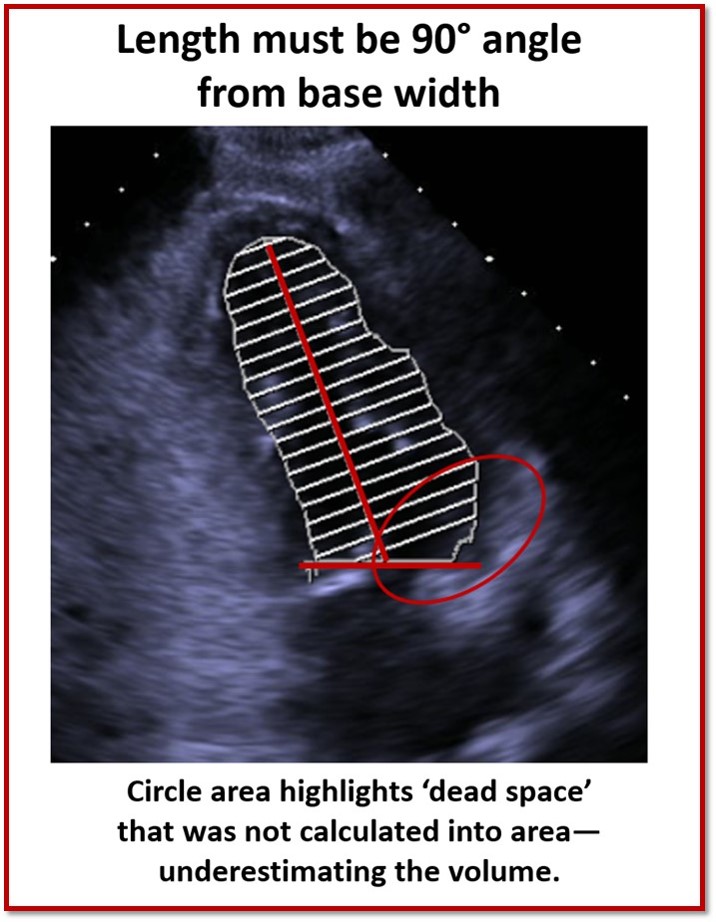
- Make sure LV length is perpendicular to base width
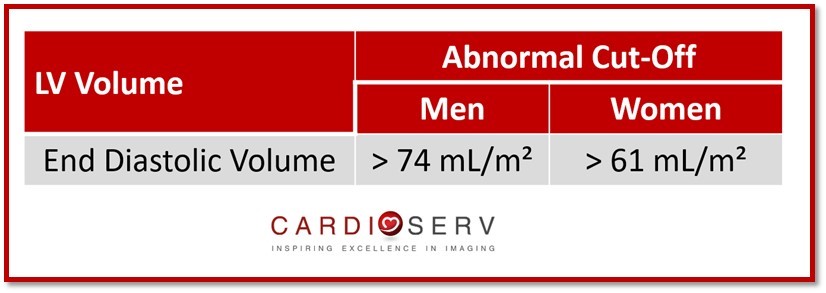
LV VOLUME VALUES
The end-diastolic (EDV) and end-systolic volumes (ESV) should be indexed to the patients BSA.

Andrea Fields MHA, RDCS
Stay Connected: LinkedIn, Facebook, Twitter, Instagram
References:
Lang, R. M., MD, Badano, L. P., MD, & Mor-Avi, V., PhD. (2015). Recommendations for Cardiac Chamber Quantification by Echocardiography in Adults: An Update from the American Society of Echocardiography and the European Association of Cardiovascular Imaging. JASE, 28(1), 1-53. Retrieved March 1, 2017, from http://asecho.org/wordpress/wp-content/uploads/2015/01/ChamberQuantification2015.pdf
Pellett, A. et al (2015) Proper Echocardiographic Measurements: How and Why. Retrieved March 1, 2017, from http://asecho.org