Last week we broke down the continuity equation to evaluate the severity of aortic stenosis. This week, we are going to discuss other methods that can be used to evaluate the severity of aortic stenosis. This blog will cover the following methods:
- AVA Planimetry
- Indexed Continuity Equation
- Velocity Ratio
These methods are recommended by the ASE in select patients when additional information is needed to evaluate the severity of aortic stenosis.
AVA PLANIMETRY
A common method to determine the aortic valve area (AVA) is by planimetry. This method is performed by manually tracing the anatomical orifice area (AOA) in the short-axis view of the aortic valve. Planimetry is recommended to be performed on transesophageal echocardiograms (TEE), rather than transthoracic (TTE).
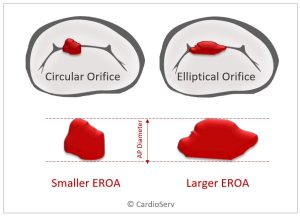
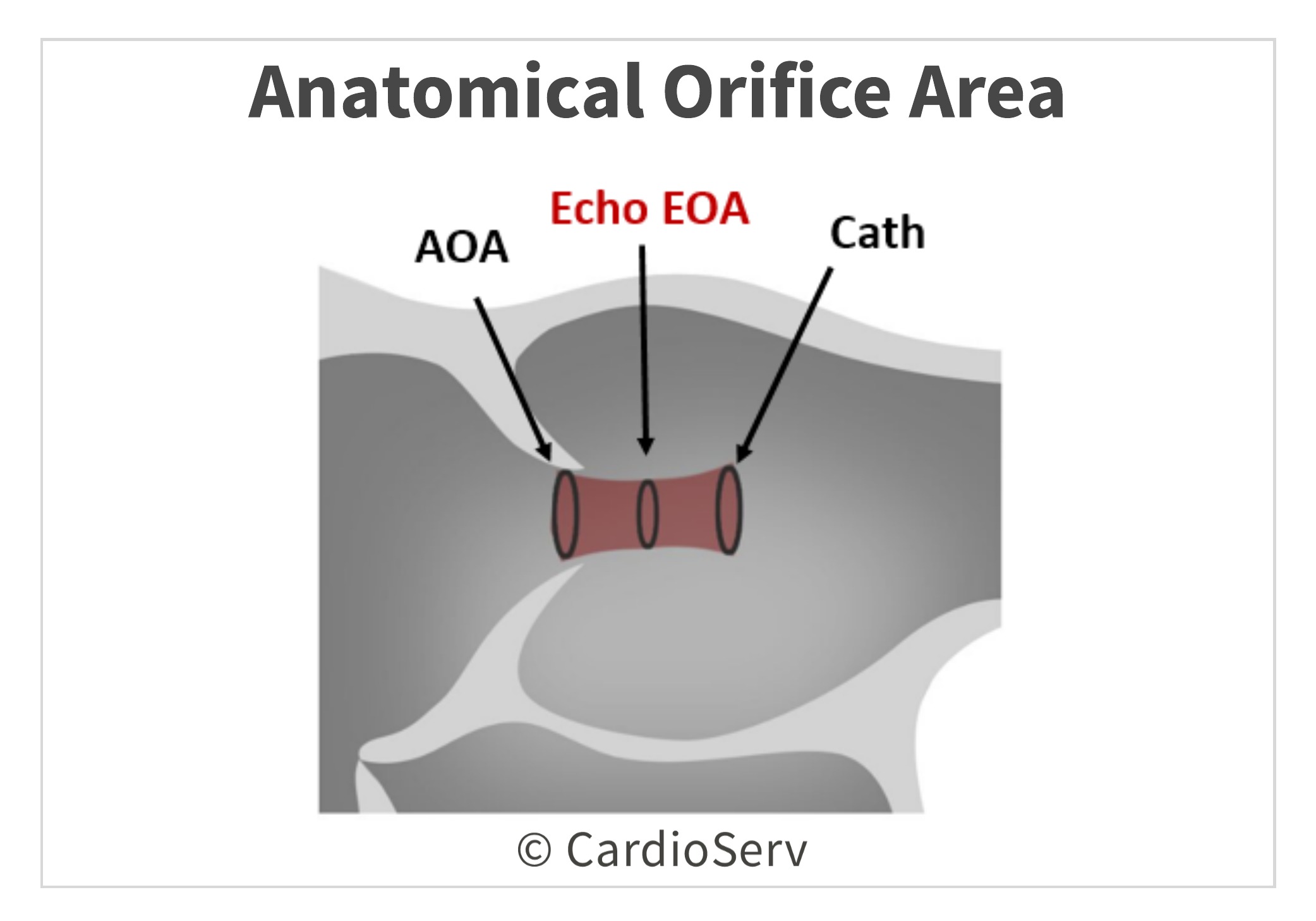
It is important to understand the manually traced AVA planimetry is not the same location as the continuity equation obtained AVA.
- The continuity equation measures the effective orifice area (EOA), which is downstream from the valve and smaller in size.
- The manually traced planimetry method measures the anatomical orifice area (AOA).
How to Perform:
- TEE preferred over TTE method
- Parasternal short-axis view
- Mid-Systole
- Trace the minimal orifice area
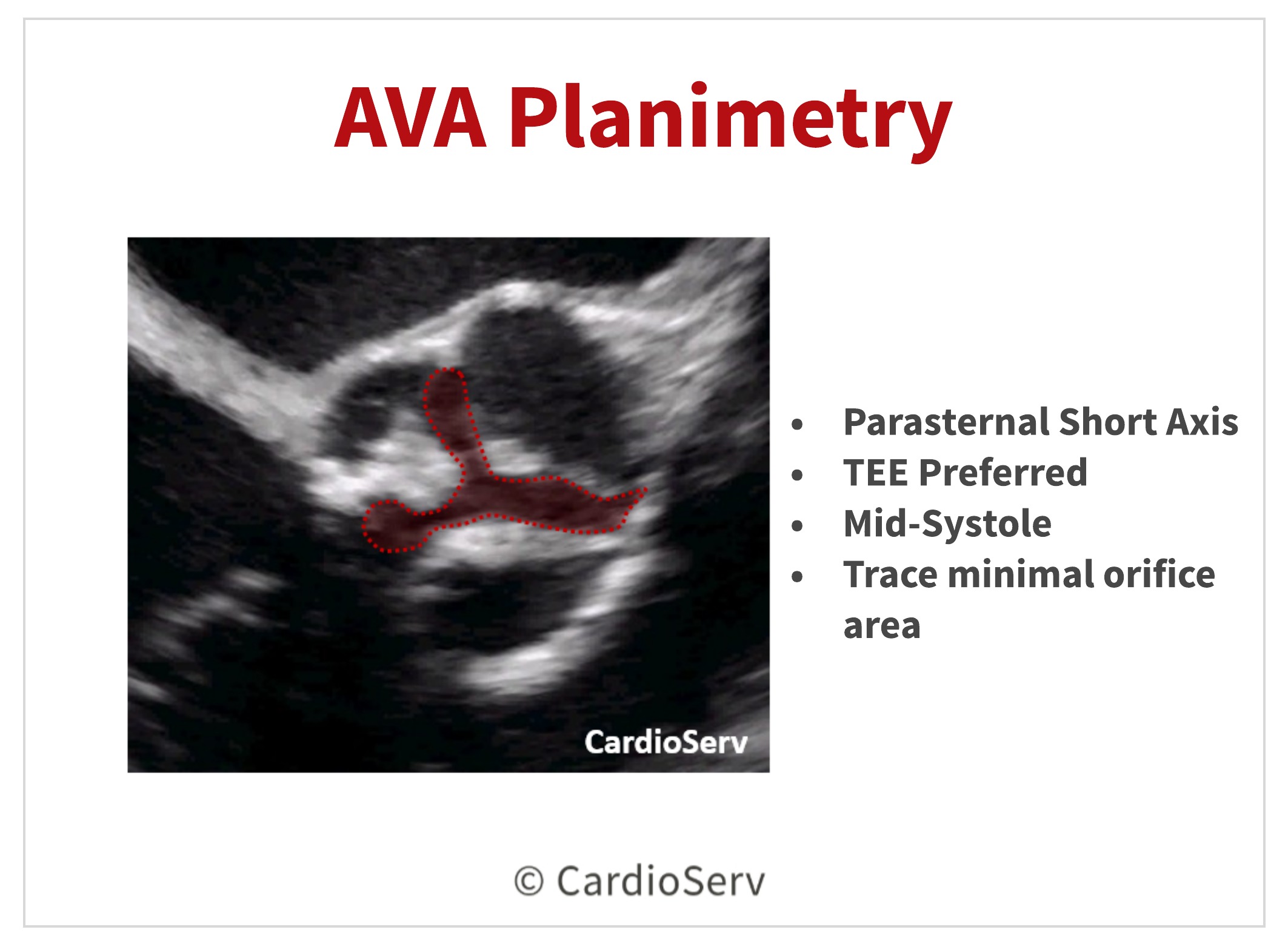
**It is vital to ensure tracing is done on the minimal orifice area and NOT the larger area proximal to the cusp tips.
Limitations:
- Challenges in accuracy of tracing due to valve calcification that causes shadows or reverberations which limits direct visualization of orifice
- Anatomical orfiice area (AOA), which is the orifice measured by planimetry, is not the primary predictor of outcome.
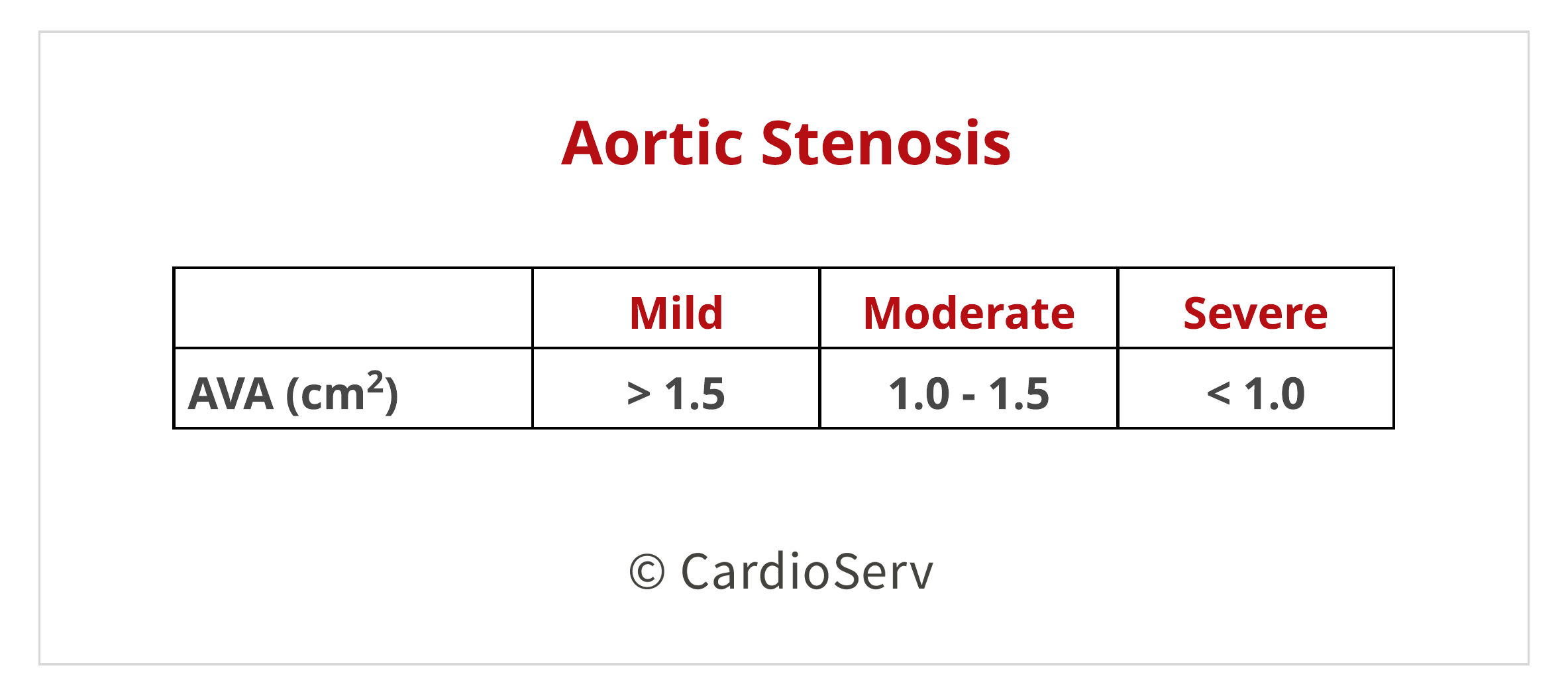
The cut-off ranges are the same for the continuity equation calculated AVA and direct tracing of planimetry.
INDEXED CONTINUITY EQUATION
Using the same steps to calculate the AVA using the continuity equation, we can take it a step further to index the AVA by body surface area (BSA). This is beneficial in select patients:
- Very large (tall) patients
- Very small (petite) patients
The BSA does not reflect the normal AVA size in obese patients. Think about it…. our valve areas do not increase with excess body weight. Only in situations where the patient is extremely tall or very petite will it affect the size of the valve.
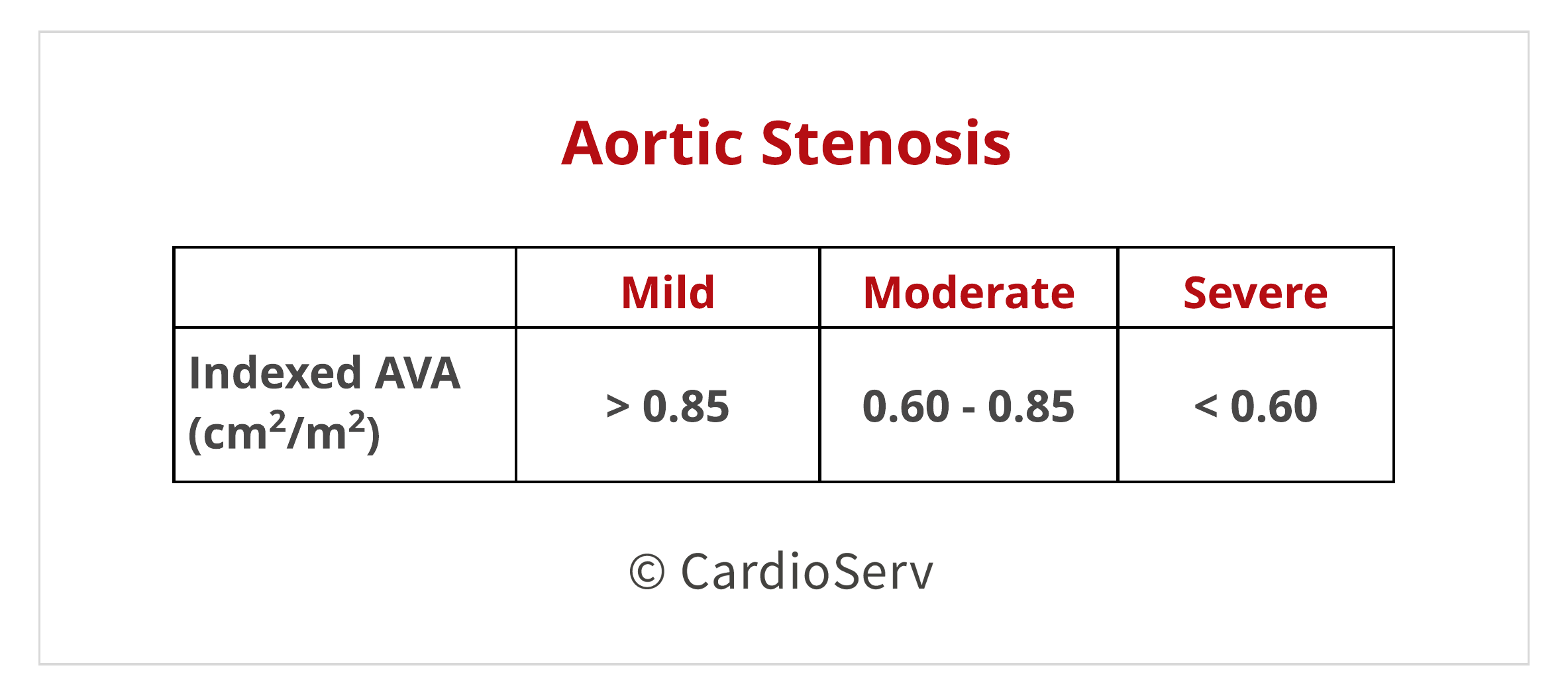
The cut-off values for indexed AVA are the following:
VELOCITY RATIO
The third additional method is using the velocity ratio (also called dimensionless index). This method still measures the effective orifice area (EOA), which is the primary predictor of outcomes.
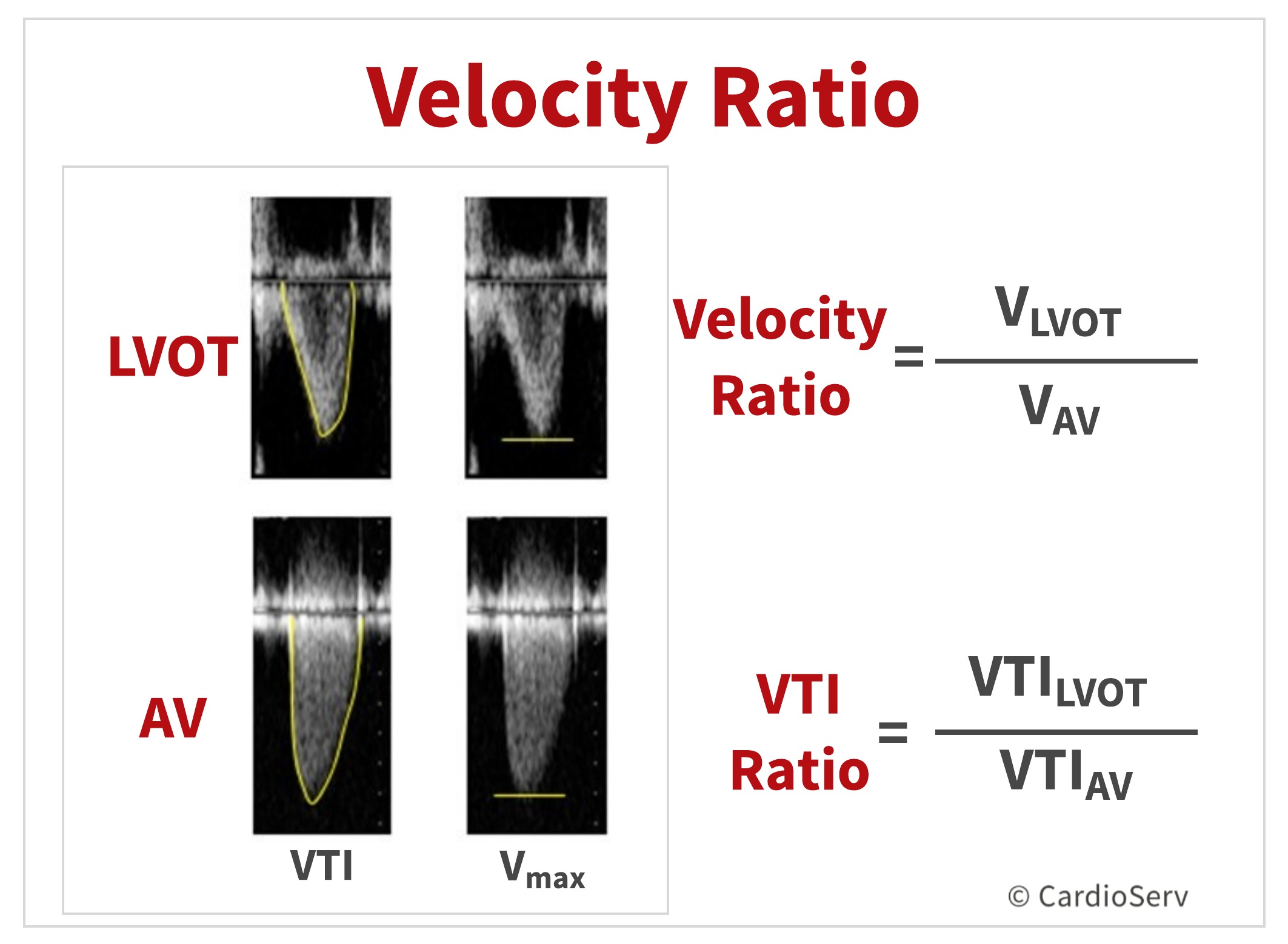
You can perform this method in 2 different ways:
- Vmax Method: Divide the LVOT Vmax by the AV Vmax
- VTI Method: Divide the LVOT VTI by the AV Vmax
The VTI method is the preferred method for evaluating the severity of aortic stenosis. Benefits of this method incude:
- Removing the assumed circular LVOT CSA from the continuity equation (which is one of the biggest potential of errors)
- Lower interobserver reproducibility from LVOT diameter
A velocity ratio less than 0.25 is suggestive of severe aortic stenosis.
SUMMARY
The evaluation of aortic stenosis with echocardiography is a very tedious task. Ensuring multiple methods are performed to enhance the accuracy of severity is critical. With echo being the gold-standard for evaluation, we need to be aware of the other methods of interrogating the valve area. The 3 additional methods discussed today are great tools to use in order to support the severity of aortic stenosis.
Check out our past blogs on aortic stenosis!
- Top 5 Factors to Consider when Evaluating for AS
- Aortic Stenosis: Breaking Down the Continuity Equation
- 4 Errors to Avoid when Measuring Aortic Valve Velocity
- Helpful Tips to Mastering the Pedoff Probe!
- Back to Basics: Aortic Valve Anatomy
- How to Master Aortic Measurements with These 5 Techniques
Want to earn Cat. 1 AMA ECHO CMEs?! Access them HERE!

Andrea Fields MHA, RDCS
Stay Connected: LinkedIn, Facebook, Twitter, Instagram
References:
Baumgartner, H., Hung, J., Bermejo, J., Chambers, J. B., Edvardsen, T., Goldstein, S., . . . Otto, C. M. (2016). Recommendations on the echocardiographic assessment of aortic valve stenosis: A focused update from the European Association of Cardiovascular Imaging and the American Society of Echocardiography. European Heart Journal – Cardiovascular Imaging, 18(3), 254-275. doi:10.1093/ehjci/jew335
Nakatsuma, K., Taniguchi, T., Morimoto, T., Shiomi, H., Ando, K., Kanamori, N., . . . Kimura, T. (2017). Prognostic Impact of Peak Aortic Jet Velocity in Conservatively Managed Patients With Severe Aortic Stenosis: An Observation From the CURRENT AS Registry. Journal of the American Heart Association,6(7). doi:10.1161/jaha.117.005524