In earlier blogs we discussed calculating the left ventricular mass (LVM) via the 2D Linear Cubed Method with assumes an ellipse shape with a major/minor axis ratio of 2:1. We received a follow up question from a reader: “Can you please provide the reference for NOT using cube method formula when major minor axis ratio is distorted?”
Thank you for the request, we’d love to provide some additional information. The ASE guidelines do provide information on calculating the LVM via the truncated ellipsoid 2D method. We will review the step by step method for this formula. Unfortunately this method is also problematic in the presence of shape distortions. The recommendation from ASE is to report LVM in hypertensive patients with a normally shaped LV via either the Linear Cubed M-Mode method or the 2D truncated ellipsoid method. “In labs that use 3D echo routinely 3D LVM should be considered – especially in abnormally shaped ventricles with asymmetric or localized hypertrophy”.
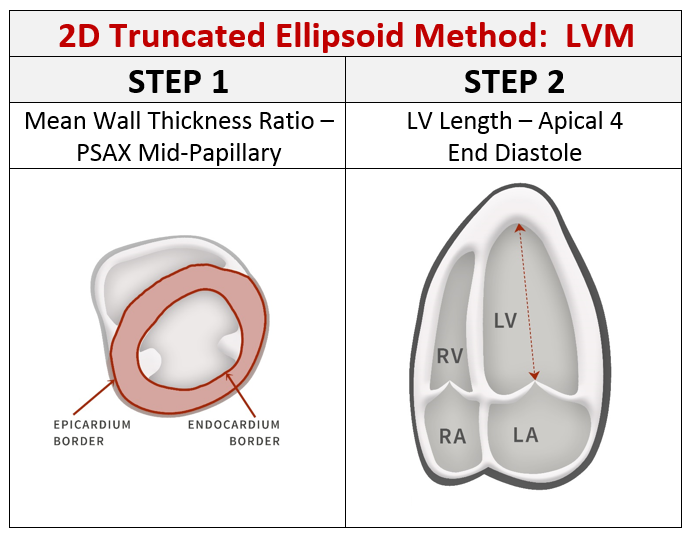
2D TRUNCATED ELLIPSOID
This method is performed in two steps! If your machine is not setup with the proper measurement calculations for these specific values, then contact your vendor to add them.
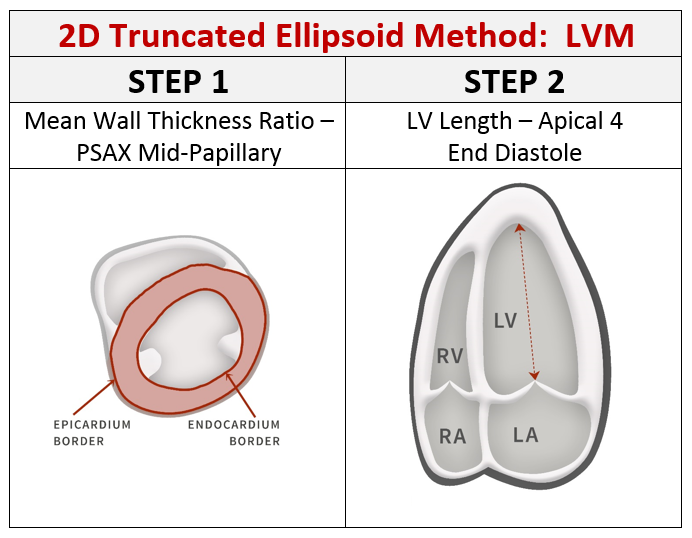
STEP 1: MEAN WALL THICKNESS RATIO
- Parasternal short axis (PSAX) at mid-papillary level
- Trace the epicardial (‘LVAd Epi’) and endocardial (‘LVAd Endo’) areas (cm²)
- Do NOT trace the papillary muscles – the papillary muscle are considered part of the LV cavity
STEP 2: LV LENGTH
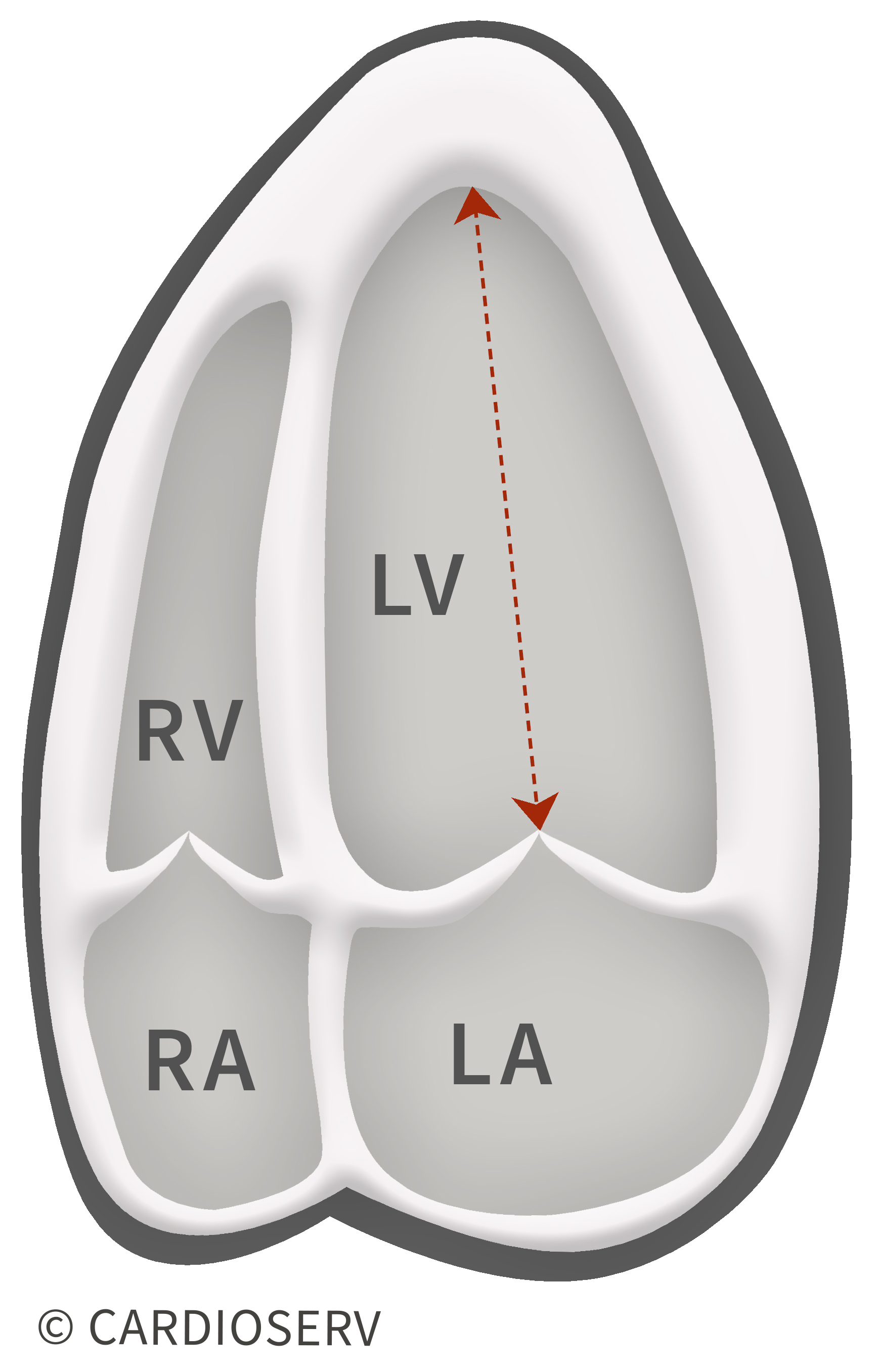
In the apical 4 chamber view
- Zoomed LV
- End-diastole
- Measure the length from the apex to base of ventricle (cm).
Your ultrasound machine should perform the calculation if you select the 2D truncated ellipsoid method when entering these values into the measurement package and should display thee LVM indexed with BSA.
REFERENCE RANGE

ADVANTAGES:
- Partial correction for shape distortions
- Less dependent on geometrical assumptions than the linear measurements
LIMITATIONS:
- Good image quality and properly oriented parasternal short-axis views (no oblique planes) are required
- Good epicardial definition is required
- Cumbersome methodology
- Higher measurement variability
- Few published normative data
- Limited prognostic data
3D ECHOCARDIOGRAPHY
The American Society of Echocardiography reminds us in the latest guidelines that 3D Echocardiograhy is the only echocardiographic technique that measures myocardial volume directly, without geometric assumptions regarding LV shape and distribution of wall thickening. Therefore this technique is promising and may be used in abnormally shaped ventricles or in patients with asymmetric or localized hypertrophy. Unfortunately, limited upper normal limits of 3D echocardiographic LV mass data are currently available in the literature but are insufficient to substantiate recommendations for reference values.
Be sure to check out our earlier blogs related to LVH:
- Understanding LVH: Concentric, Eccentric and Concentric Remodeling
- How to measure LV Mass and diagnose LVH
- Should LVM be indexed with height or BSA?
YOU ASKED….WE ANSWERED! CONNECT WITH US ON SOCIAL MEDIA SO YOU CAN BE PART OF THE CONVERSATION!
References
- https://acc.org/latest-in-cardiology/articles/2016/02/02/08/21/approaches-to-echocardiographic-assessment-of-left-ventricular-mass?w_nav=Tab
- Marwick, T. H., PhD, Gillebert, T. C., MD, & G. A., MD. (2015). Recommendations on the Use of Echocardiography in Adult Hypertension. JASE,28(7), 1-12. Retrieved March 1, 2017, from http://asecho.org/wordpress/wp-content/uploads/2015/07/2015_Hypertension.pdf
- Lang, R. M., MD, Badano, L. P., MD, & Mor-Avi, V., PhD. (2015). Recommendations for Cardiac Chamber Quantification by Echocardiography in Adults: An Update from the American Society of Echocardiography and the European Association of Cardiovascular Imaging. JASE, 28(1), 1-53. Retrieved March 1, 2017, from http://asecho.org/wordpress/wp-content/uploads/2015/01/ChamberQuantification2015.pdf