Last week we discussed clear & easy tips on how to evaluate different abnormalities of the mitral valve (MV) for primary MR. We also explained the Carpentier’s Classification concept and how it’s applied to various etiologies of the MV. If you need to refresh or missed our past blogs, you can find them here:
- Mitral Valve Anatomy: Name 5 Components!
- Finally… Mitral Valve Orientation Explained!
- Smart Strategies for Determining MR Mechanisms
- Ultimate Guide to Acute vs. Chronic MR
- Essential Steps to Evaluating MR Etiologies
SECONDARY/FUNCTIONAL MR
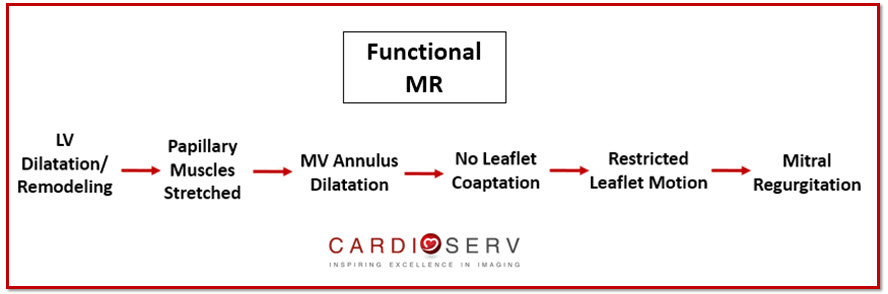
In our prior MV mechanism blog we discussed how secondary MR is due to the disease of the left ventricle, not from leaflet abnormality. How does this cause MR? Let’s break it down:
- LV becomes dilated
- Papillary muscles become stretched & displaced
- Mitral annulus becomes dilated
- Mitral leaflets become restricted
- Leaflets fail to coapt properly
- Tethering motion of leaflets occur
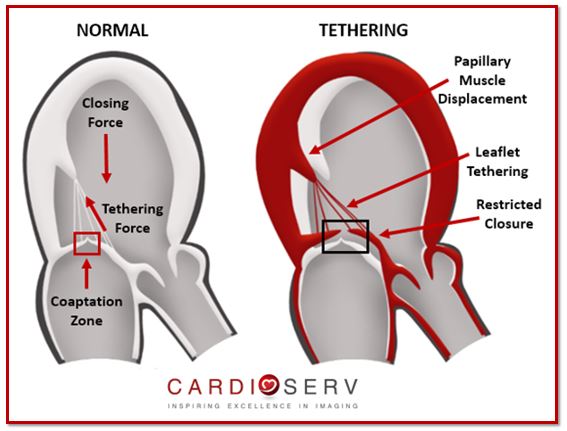
When the LV dilates the papillary muscles become stretched and displaced, which causes dilatation of the MV annulus. This causes the leaflets to become restricted during systole and not properly coapt (leaflets motion then tethers), causing the regurgitation.
Therefore, MV leaflet tethering is a result of secondary/functional MR occurring. It describes the motion of the leaflets due to dilatation of LV and mitral annulus, restricted motion and failure of leaflet coaptation. Carpentier’s Classification of secondary MR is usually Type IIIb.
ETIOLOGIES OF MITRAL VALVE TETHERING
Tethering, due to secondary MR, can be broken down into 2 categories: ischemic & non-ischemic.
- Ischemic: The result of LV remodeling post-myocardial infarction (MI).
- Non-Ischemic: Commonly due to chronic cardiomyopathies, such as hypertensive or dilated.
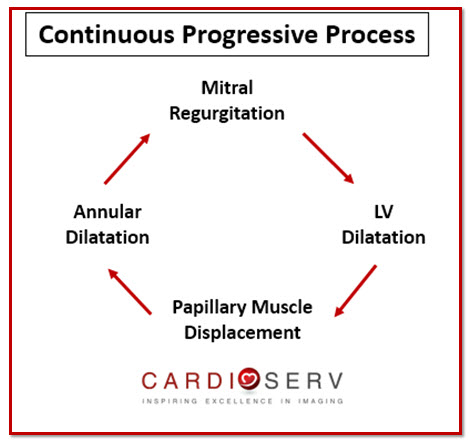
Remember the regurgitation is due to the disease of the left ventricle, not the leaflets. Without surgical intervention, overtime the severity of MR will increase due to a continuous on-going process of cardiac remodeling. As the MR remains present, the LV will continue to dilate to compensate for volume overload, which will cause continual displacement of papillary muscles. This will stretch the leaflets more, dilating the annulus and creating more regurgitation.
TYPES OF MITRAL VALVE TETHERING
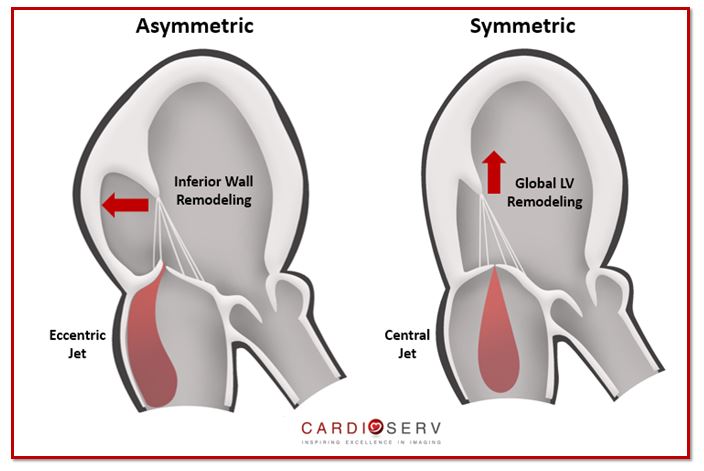
Tethering can occur in two different ways:
- Symmetric Tethering- both leaflets tether causing global LV systolic dysfunction & remodeling with a centrally directed MR jet
- Asymmetric Tethering- one leaflet tethers due to localized remodeling & dysfunction of posterior wall with an eccentrically posterior directed MR jet
- Most commonly type found
- Systolic leaflet restriction of posterior leaflet
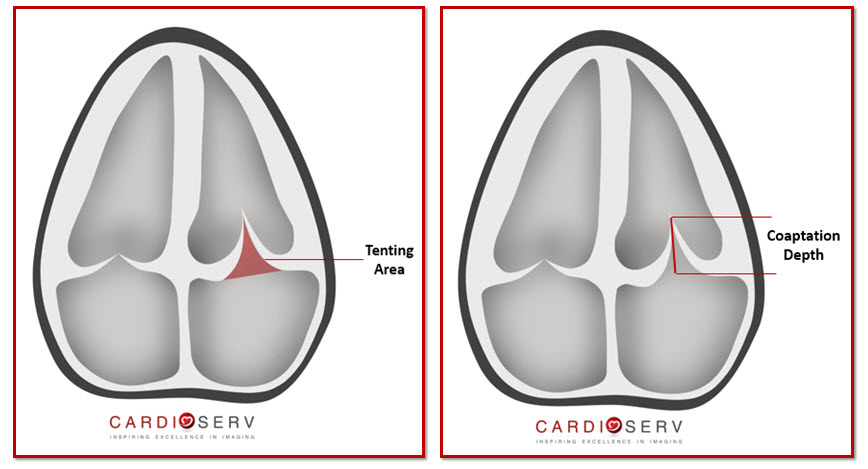
HOW TO IMAGE: MITRAL VALVE TETHERING
NOTE: Measurement of leaflet coaptation are not accurate with TTE. The measurements do not classify further into mild, moderate or severe.
Coaptation depth = Measures the maximal distance from leaflet tips to annular plane
Tenting Area = Area measurement from leaflet tips to annular plane during mid-systole (area is at minimum)
SUMMARY
Our goal by the end of this blog is to properly identify and evaluate mitral valve tethering.
As physicians, sonographers & healthcare clinician’s–we need to remember the importance of identifying the mechanism & etiology that is causing the mitral regurgitation. They play a major role in the severity of the regurgitation, cardiac remodeling and management process of the patient. Stay tuned for the upcoming weeks to follow as we dig deeper into our mitral regurgitation blog series!
Our goal at CardioServ is to provide you with an easy process of understanding and properly evaluating mitral regurgitation! We look forward to hearing feedback and comments from our readers!

Andrea Fields MHA, RDCS
Stay Connected: LinkedIn, Facebook, Twitter, Instagram
References:
Jouan, J. (2014). Mitral Valve Repair Over Five Decades. Annals of Cardiothoracic Surgery,4(4), 322-335. Retrieved July 6, 2017, from http://www.annalscts.com/article/view/6825/7706
Asgar, A. W., Mack, M. J., & Stone, G. W. (2015). Secondary Mitral Regurgitation in Heart Failure. Journal of the American College of Cardiology,65(12), 1231-1249. Retrieved July 6, 2017, from http://www.onlinejacc.org/content/65/12/1231?_ga=2.101757569.1871068379.1498150942-2075798501.1487771433
Saito, K., Okura, H., Watanabe, N., Obase, K., & Tamada, T. (2012). Influence of Chronic Tethering of Mitral Valve on Mitral Leaflet Size and Coaptation in Functional Mitral Regurgitation. Jour,5(4), 337-344. Retrieved July 6, 2017, from http://www.imaging.onlinejacc.org/content/5/4/337?_ga=2.169400609.1871068379.1498150942-2075798501.1487771433
Dal-Bianco, J. P., MD, Aikawa, E., MD, Bischoff, J., PhD, Guerrero, J. L., BS, & Hjortanes, J., MD. (2016). Myocardial Infarction Alters Adaptation of the Tethered Mitral Valve. Journal of the American College of Cardiology,67(3), 275-288. Retrieved July 6, 2017, from http://www.onlinejacc.org/content/67/3/275?_ga=2.126940813.1871068379.1498150942-2075798501.1487771433
Zoghbi, W. A., MD, FASE, & Adams, D., RCS, RDCS, FASE. (2017). Recommendations for Noninvasive Evaluation of Native Valvular Regurgitation. JASE, 30, 4th ser., 1-69. Retrieved June 12, 2017.