Pulmonary embolism (PE) is a critical condition where one or more of the arteries within the lungs become occluded by a blood clot. Quick diagnosis and treatment is crucial to keep mortality rates low. It is common for PE’s to originate from lower limb deep venous thrombosis (DVT). In other words: PE’s can occur due to severe complications of DVTs. There are over 600,000 cases of PE’s annually within the United States; 79% present with evidence of DVT.
But wait! – How can a thrombus in a vein become a thrombus in an artery?
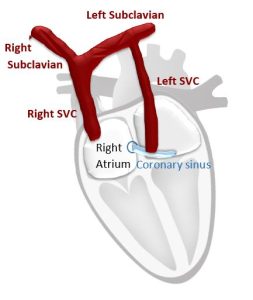
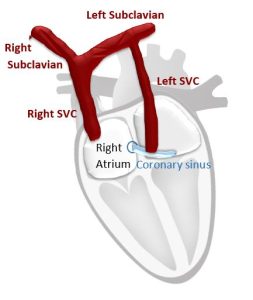
Lets think about the circulatory system…
- Deoxygenated blood travels within the inferior vena cava (IVC) to the heart to become oxygenated.
- IVC pushes the deoxygenated blood into the right atrium (RA) to the right ventricle (RV).
- The blood is sent to the lungs via the pulmonary artery (PA) to receive good oxygenated blood!
- Once it becomes oxygenated, it is sent to the left side of the heart and out through the aorta to entire body!
Now let’s walk through how a DVT turns into a PE:
- Thrombus forms in the proximal femoral vein (DVT).
- DVT travels proximal within the IVC to the right heart.
- Deoxygenated blood & DVT travel to the pulmonary artery & into the lungs.
- The thrombus blocks one or more of the arteries within the lungs, causing a PE to occur.
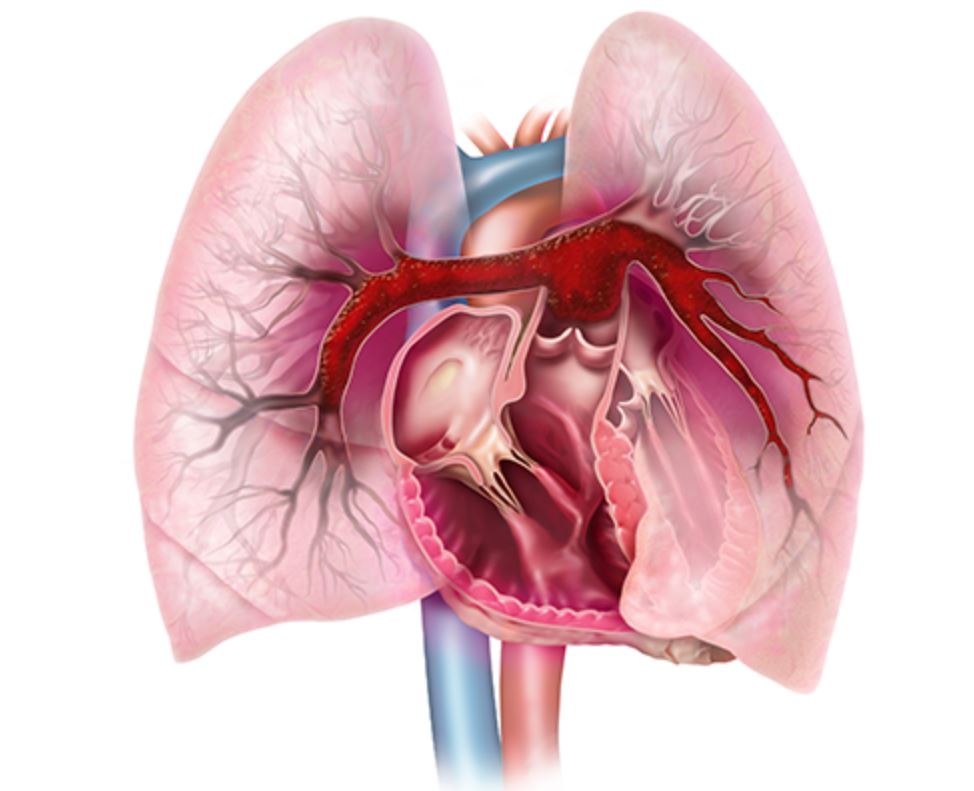
Image From EKOS: https://www.btg-im.com/en-US/EKOS/Home
PULMONARY EMBOLISMS EFFECTING THE HEART
The size and location of the PE effects the size and function of the heart. The embolism becomes obstructed within the right ventricular outflow tract (RVOT), preventing blood to reach the lungs to become oxygenated. This causes a sudden pressure change in the right heart:
- Acute dilatation of right ventricle
- Acutely elevated pressures
- McConnell Sign (read about this echo-specific finding on our prior blog here!)
CLASSIFYING PULMONARY EMBOLISMS
We are able to classify PE’s into various categories to help determine the mortality and prognosis rates. The classification is determined based on the estimated early death risk. This concept helps determine the patients clinical course of treatment and risk of adverse outcomes. It involves the presence of:
- Right ventricular dysfunction
- Right heart failure
- Pressure overload
The presence of RV dysfunction on echo was associated with a mortality rate of 57% at 3 months, regardless of the patients hemodynamic state. The RV/LV ratio >0.9 is another predictor of hospital mortality.
The three classifications for PE’s include:
- Massive PE
- Present with shock or arterial hypotension due to right heart failure
- High Risk
- 5% PE Population
- 58% Mortality at 3 Months
- Submassive PE
- Present hemodynamically stable but have evidence of RV dysfunction & positive biomarkers
- Moderate/Intermediate Risk
- 40% PE Population
- 2-21% Mortality at 3 Months
- Minor PE
- Present with stable hemodynamics and negative biomarkers
- Low Risk
- 55% PE Population
- Low Mortality Rate
Treatment of submassive and massive PE include anticoagulation treatment over the course of 3 months. If treatment is started at a reasonable time from onset of symptoms, improvement of right heart function and pressures will occur within 36 hours.
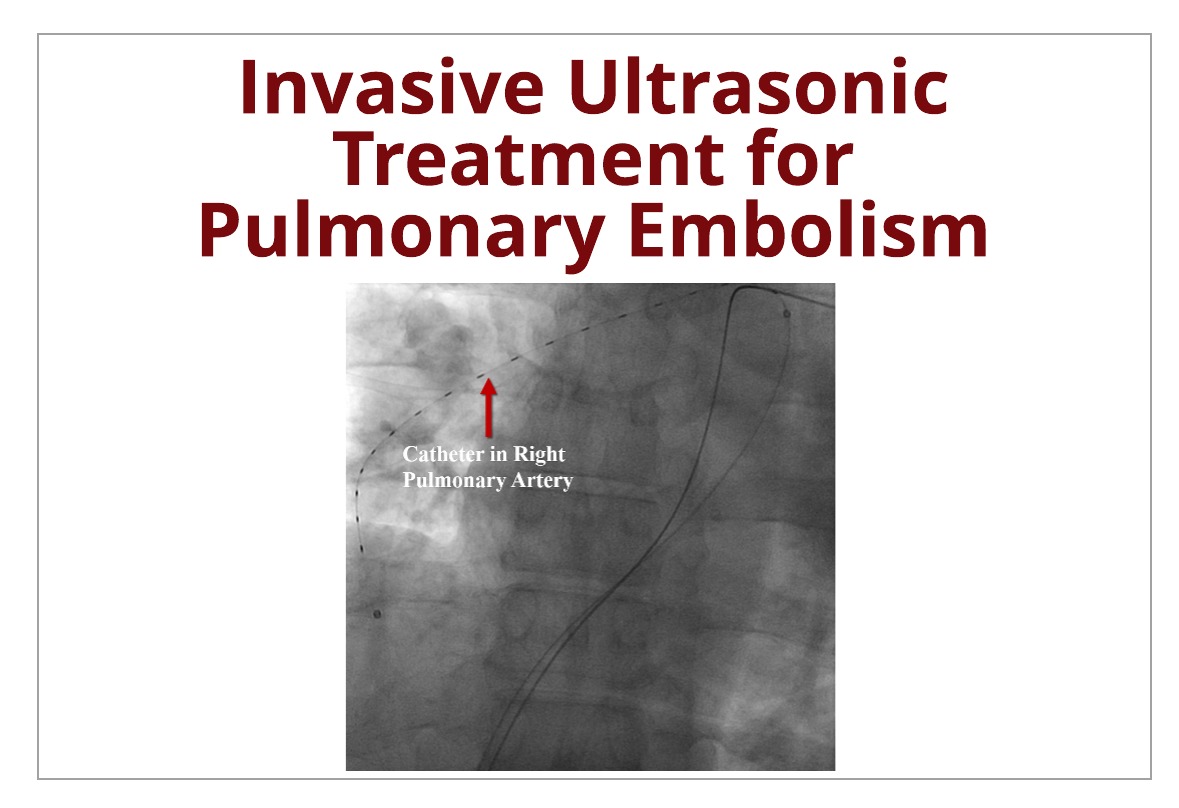
INVASIVE CATHETER TREATMENT FOR PULMONARY EMBOLISM
New technology has allowed the development of an invasive catheter approach to treating PE’s at a faster rate. EKOS Acoustic Pulse Thrombolysis is a invasive catheter that uses ultrasonic waveforms to directly deliver anticoagulant drug to thrombus site.
Basically this procedure places a catheter in the vessel and through the blood clot and left in that specific position while the catheter emits ultrasonic sound waves and a thrombolytic agent. The sound waves performs two functions.
- Generates radial pressure that drives the lytic drugs into the inner portions of the clot
- Thins the fibrin within the clot
Delivering the drug this way allows the lytic treatment to infiltrate the clot more efficiently enabling a faster rate for of thrombus dissolution with less drug dosage!
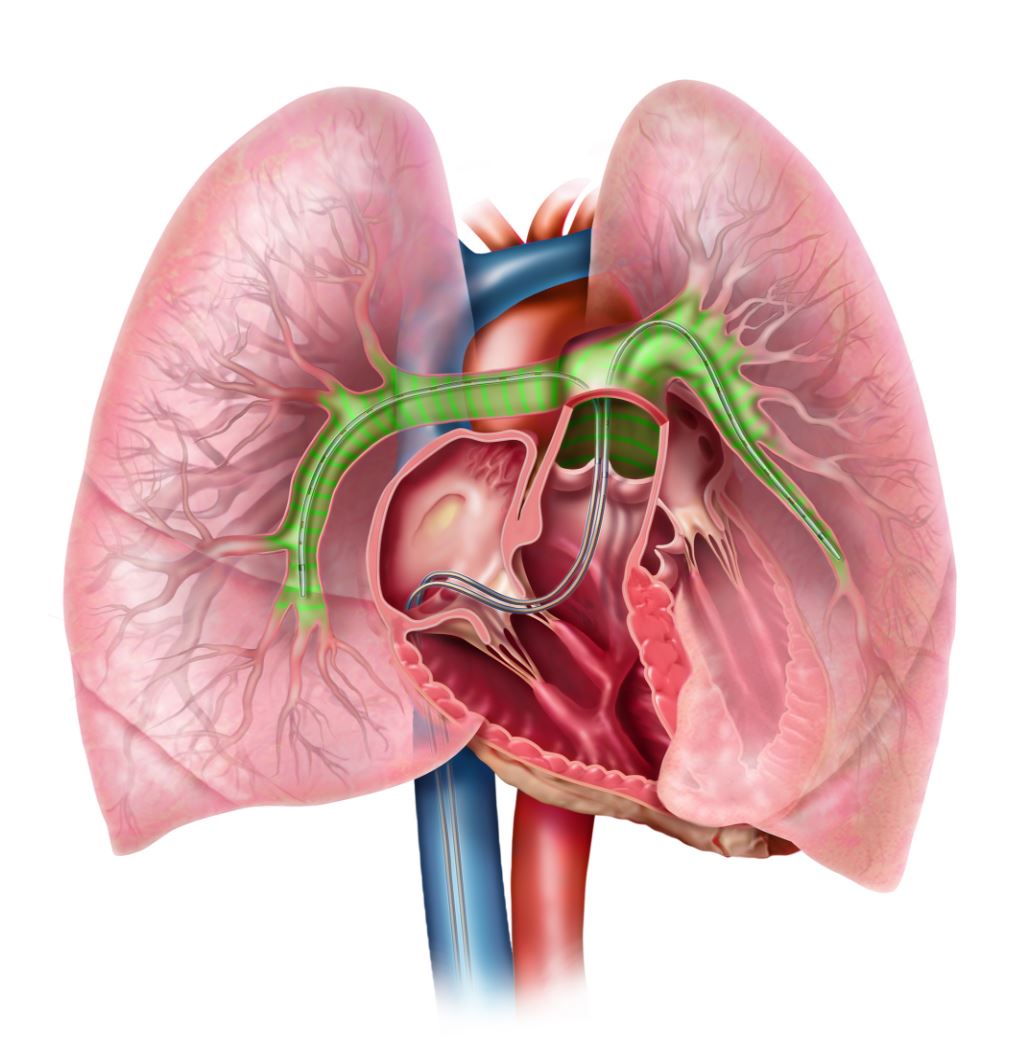
Image From EKOS: https://www.btg-im.com/en-US/EKOS/Disease-states/Pulmonary-Embolism
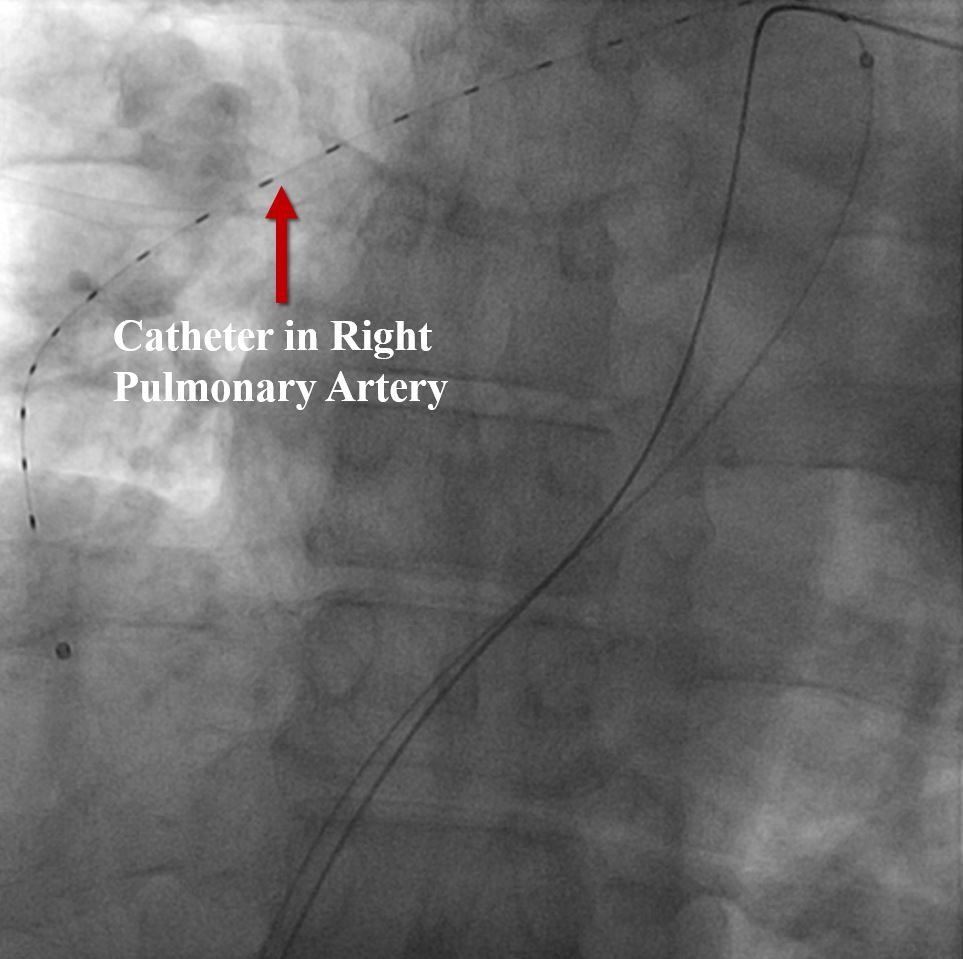
EKOS allows for a fast, efficient process to rapidly treat acute, submassive and massive PE’s. The procedure allows quick treatment to the thrombus in a few steps:
- Catheter inserted through the thrombus
- Ultrasonic core placed and locked
- Turn on lytic infusion with acoustic pulse
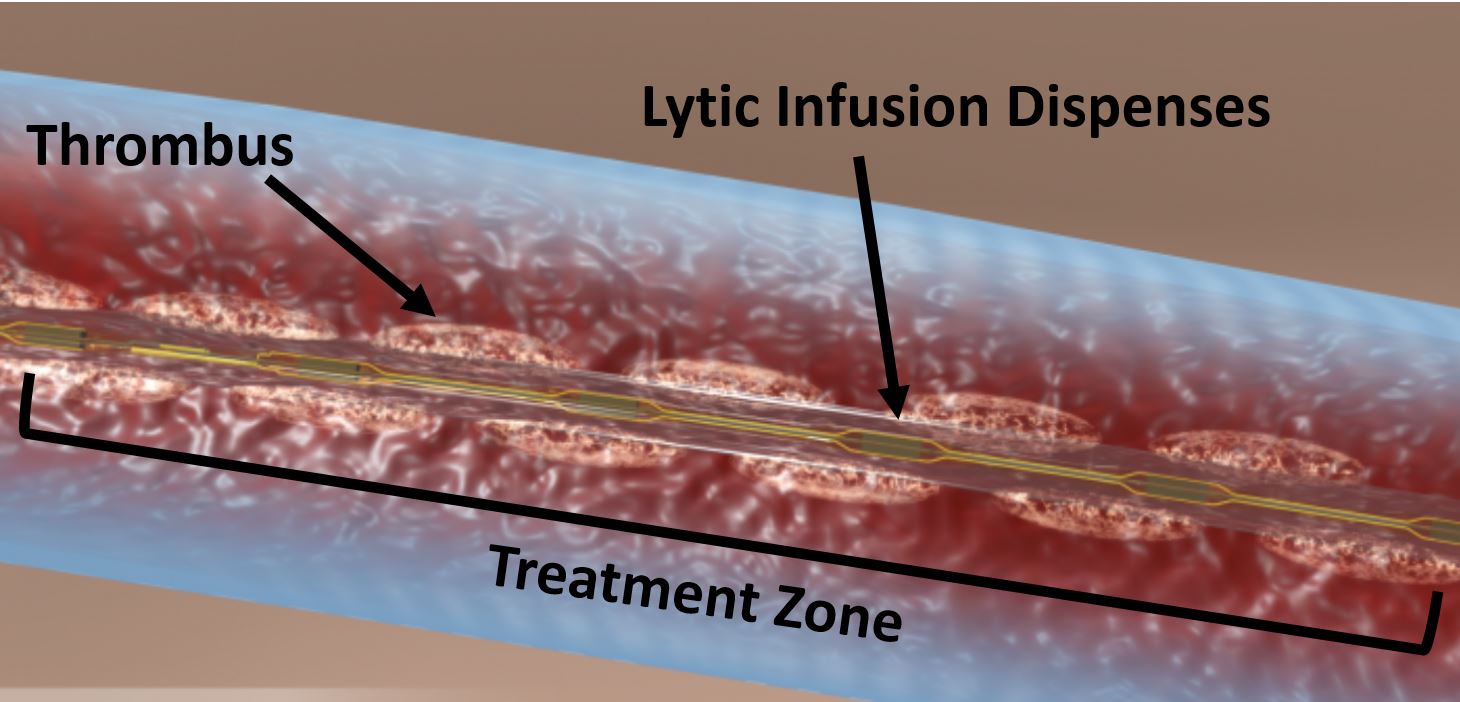
Image from DAIC: https://www.dicardiology.com/article/ultrasound-assisted-catheter-directed-thrombolysis-reduces-treatment-risks-pulmonary-emboli
After placement of the device in the cath lab, the patient is brought back to the ICU unit with device still in and lytic infusion running. EKOS system allows rapid reduction of RV afterload and improves the function and size of the right heart. Improvement can be seen within hours from onset of treatment. Learn more about EKOS by watching this video that explains the process of implementing EKOS system for PE. Watch Here!
CONCLUSION
Pulmonary embolism is a critical condition where one or more of the arteries within the lungs become occluded by a blood clot. As cardiologists and sonographers, we play a crucial role in the correct diagnosis and treatment of this potentially fatal condition. It is important to stay current with the latest treatment options available to our patients.
Learn more about the correct diagnosis of pulmonary embolism via echocardiography mentioned in some of our past blogs:
Need CMEs? CardioServ now offers Cat. 1 AMA Echo CMEs!


Andrea Fields MHA, RDCS
Stay Connected: LinkedIn, Facebook, Twitter, Instagram
References:
http://www.acc.org/latest-in-cardiology/ten-points-to-remember/2016/02/22/12/40/management-of-pulmonary-embolism-an-update