As we come to an end with our right heart blog series, we want to conclude with a comprehensive look at the role of hepatic vein evaluation to assess the right heart. We will break this down into 2 blogs this week. This first blog will cover the fundamentals of hepatic veins and the second part will review how the hepatic veins play a role in Tricuspid regurgitation (TR) and right heart failure.
We are going to discuss the fundamentals of hepatic veins, and how they relate to the heart. This blog will review:
- Function of the hepatic veins
- Hepatic waveform flow patterns
- Hepatic waveforms and the cardiac cycle
- Pathology identified with the evaluation of the hepatic veins
- Identifying normal and abnormal waveforms
1. FUNCTION OF THE HEPATIC VEINS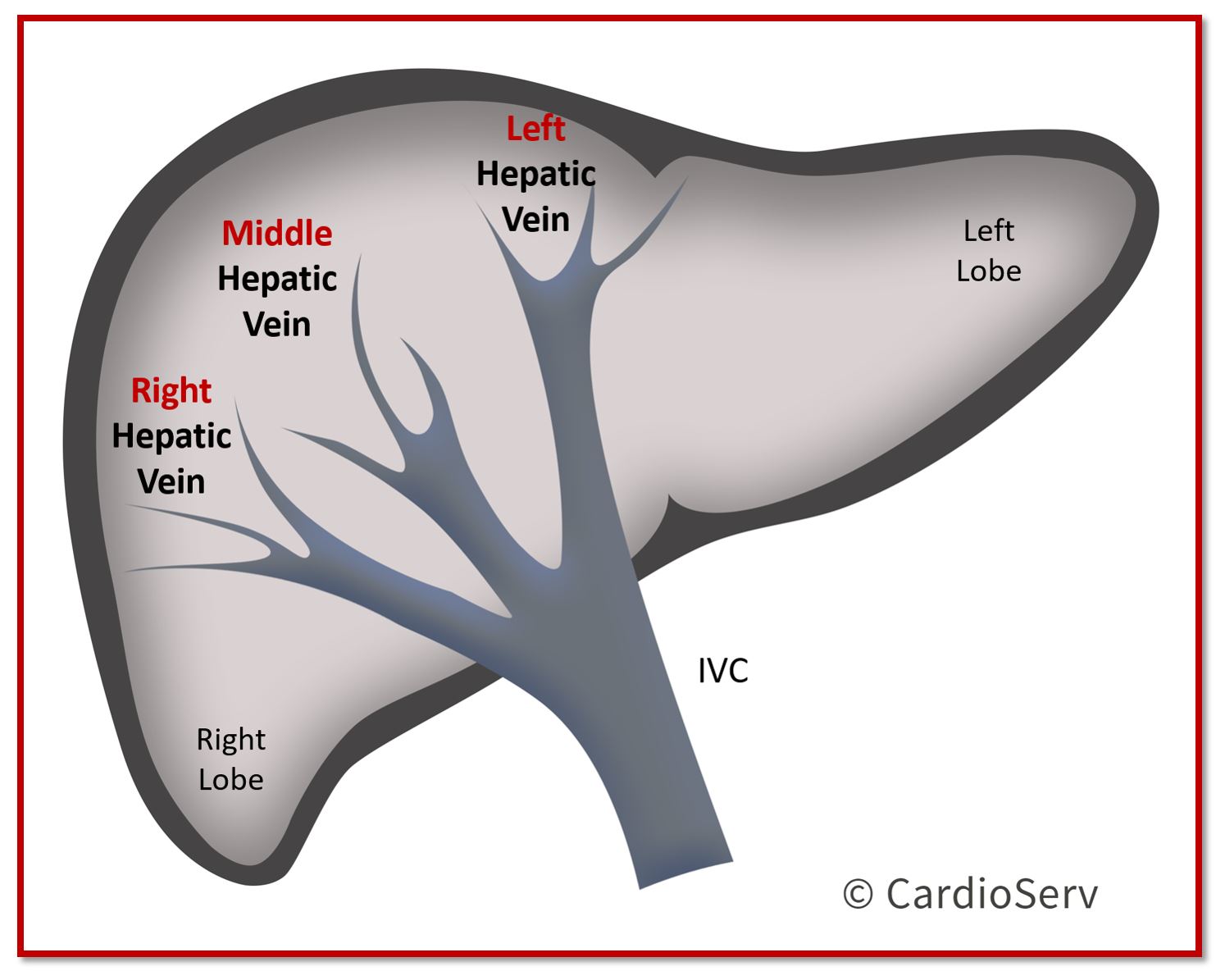
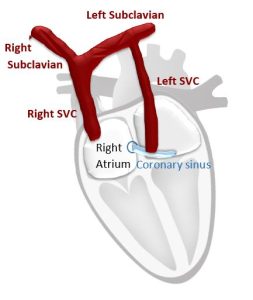
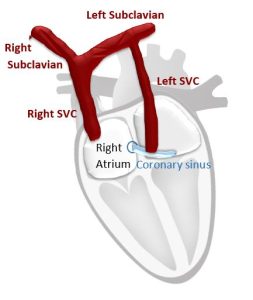
The hepatic veins transport deoxygenated blood from the liver to the inferior vena cava (IVC), which pumps the blood into the right atrium. From there, the right heart delivers the deoxygenated blood through the pulmonary artery (PA) to the lungs in order for the blood to get oxygenized!
- Blood flows towards IVC and heart
- Away from transducer, represented by blue color Doppler
- Represents the venous pressure transmitted from right ventricle (RV)
- 3 Veins: Right Hepatic, Middle Hepatic, Left Hepatic
- Tetraphasic waveform pattern
- Normal size <10 mm (at proximal site of IVC)
2. HEPATIC WAVEFORM FLOW PATTERNS
When discussing the flow pattern for the hepatic veins, we must consider the blood flow pathway in regards to the circulatory system and transducer.
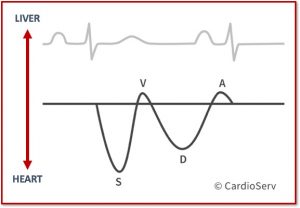
Antegrade: Flow towards the heart [away from transducer = blue]
- Represented below the baseline
Retrograde: Flow away from the heart [towards the transducer = red]
- Represented above the baseline
Hepatic Veins:
Antegrade: flow moving TOWARDS the heart
Retrograde: flow moving AWAY from heart (towards liver)
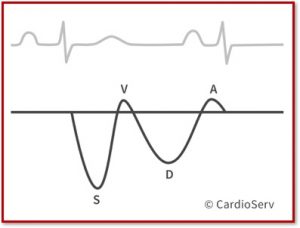
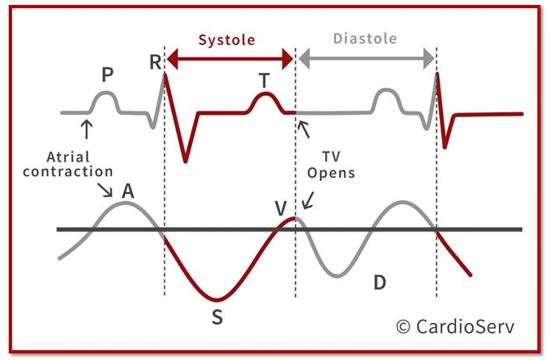
The hepatic veins are considered a phasic, predominately antegrade waveforms. They are composed of 4 parts:
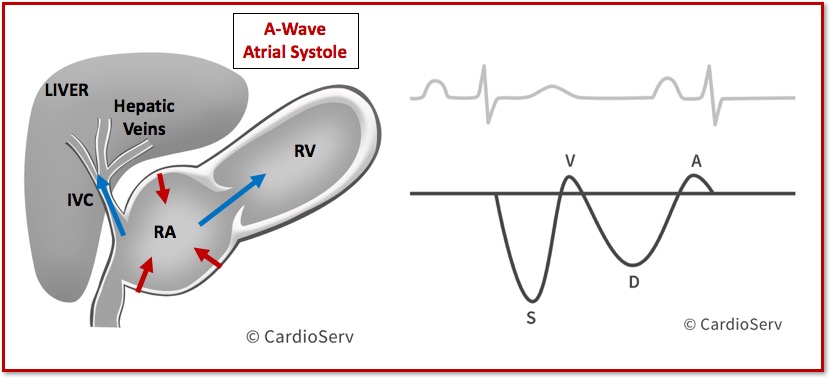
- A-Wave: Atrial Contraction (Systole)
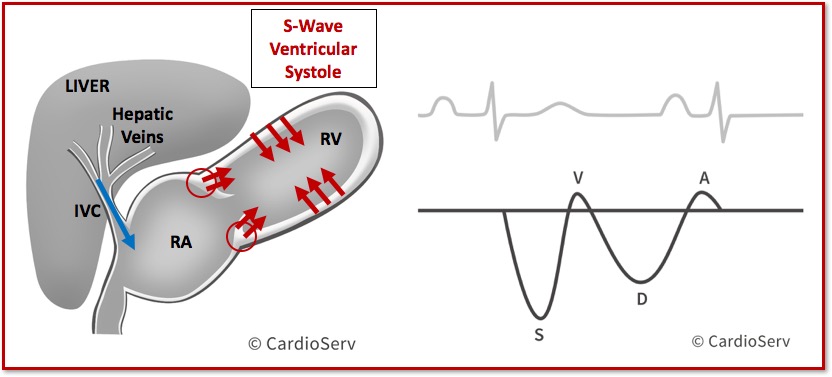
- S-Wave (Vs): Ventricular Systole
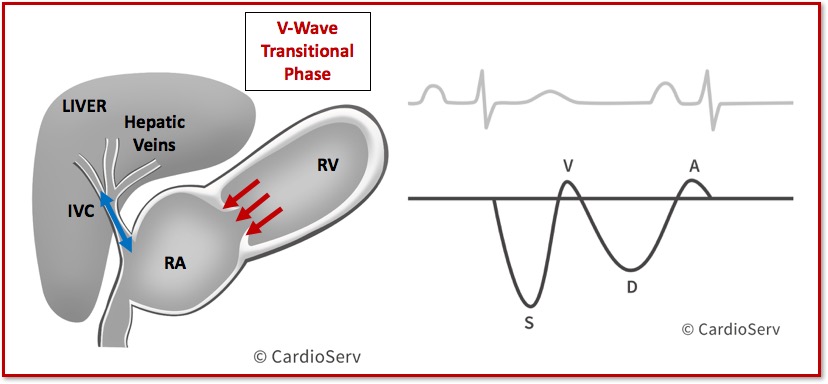
- V-Wave: Transitional Phase
- D-Wave (Vd): Ventricular Diastole
3. HEPATIC WAVEFORMS AND THE CARDIAC CYCLE
Let’s walk through each waveform and see how it relates to the cardiac cycle…
A-Wave: Atrial Systole
- Generated by increase in RAP
- Reflective upon maximum retrograde venous flow
- Tricuspid valve open
- Blood transferred in 2 directions:
- Towards RV (antegrade)
- Towards IVC/Hepatic (retrograde)
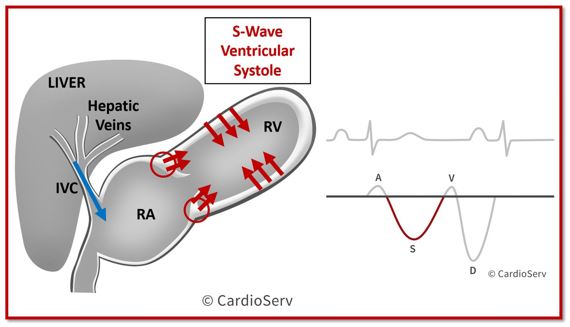
S-Wave: Ventricular Systole
- Largest amount of blood flows from hepatic veins into RA
- RV walls contract, pushing blood out into right ventricular outflow tract (RVOT)
- Tricuspid annulus moves upward, towards apex of RV
- Causes negative pressure within RA & decrease in RAP
V-Wave: Transitional Phase
- Atrial overfilling
- Tricuspid annulus returns to resting position
- Decrease in blood filling into RA and blood flow velocities toward heart
D-Wave: Ventricular Diastole
- Tricuspid valve opens
- RA and RV fill passively
- Antegrade flow from hepatics to RA
- Decrease in RAP due to early rapid diastolic filling of right ventricle
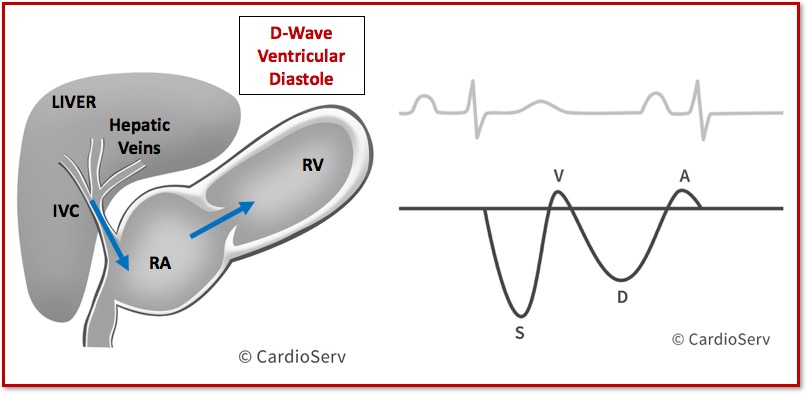
To help with putting all this information together, take a look at this image:
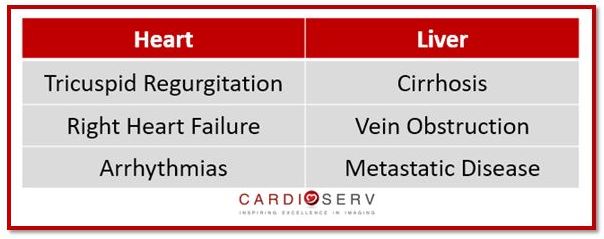
4. PATHOLOGY IDENTIFIED WITH EVALUATION OF THE HEPATIC VEINS
The hepatic veins can give us lots of information regarding both heart and liver abnormalities. Below is a short list of common abnormalities, that evaluation of hepatic veins can help diagnose:
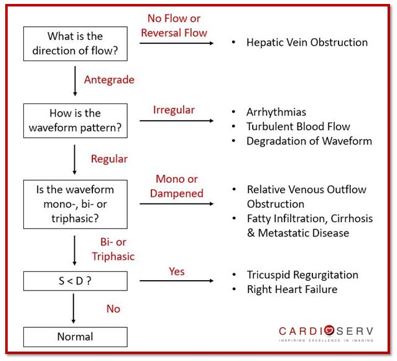
5. IDENTIFYING NORMAL AND ABNORMAL WAVEFORMS
When we look at the hepatic vein Doppler, we need to evaluate the waveform patterns and velocities. We should ask ourselves these questions to determine if the waveform is normal or abnormal:
- What is the direction of flow seen?
- How does the waveform pattern appear?
- What is the phasicity of the waveform?
- Is the D-wave larger than the A-wave?
CONCLUSION
This week we are closing out our right heart blog series with a 2-part discussion of the hepatic veins. Here, in part 1 we reviewed the function and waveform patterns of the hepatic veins. We commonly forget the importance of the hepatic veins in regards to the right heart. In part 2 of this blog topic, we are going to discuss how the hepatic veins help determine severity of tricuspid regurgitation and right heart failure!
WANT A CME FOR READING THIS BLOG? CLICK BELOW TO ACCESS CARDIOSERV’S ONLINE CME PLATFORM OFFERING CAT. 1 AMA CMES!


Andrea Fields MHA, RDCS
Stay Connected: LinkedIn, Facebook, Twitter, Instagram
References:
Scheinfield, M. H., MD, Bilali, A., ARDMS, & Koenigsberg, M., MD. (2009). Understanding the Spectral Doppler Waveform of the Hepatic Veins in Health and Disease. RadioGraphics,29, 2081-2098. Retrieved May 31, 2017, from http://pubs.rsna.org/doi/pdf/10.1148/rg.297095715
Rudski, L. G., MD. (2010). Guidelines for Echocardiographic Assessment of the Right Heart in Adults: A Report from the American Society of Echocardiography. JASE, 23, 685-713.