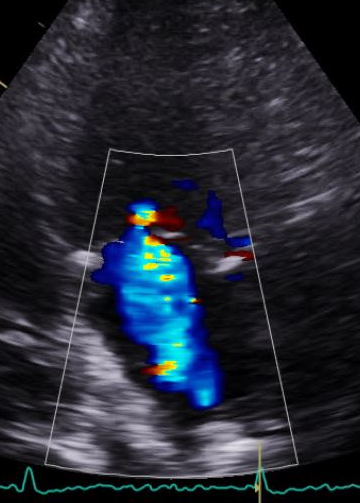
VENA CONTRACTA WIDTH (VCW)
In last week’s blog, we reviewed the correct way to measure the vena contracta width (VCW) This week we will review how MR mechanisms (primary v. secondary MR) affect the accuracy of MR vena contracta assessment.
Recap:
- Vena contracta is the narrowest portion of the MR jet
- Semi-quantitative measure
- A good marker to distinguish mild from severe
- Small measurement errors lead to misclassification of MR severity
Vena Contracta Width: Limitations
Last week, we reviewed some of the limitations of the vena contracta width which included:
- Overestimates MR: Non-holosystolic jet (MVP)
- Underestimates MR: Multiple jets
- Underestimates MR: Elliptical-shape orifice (secondary MR)
It can be easy to skim through a pro and con list without fully understanding the consequences. Let’s take a look at one of the downsides to the vena contracta width (VCW) measurement, in regards to the MR orifice shape.
MR MECHANISM AND VENA CONTRACTA SHAPE
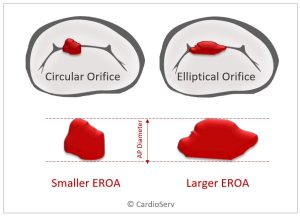
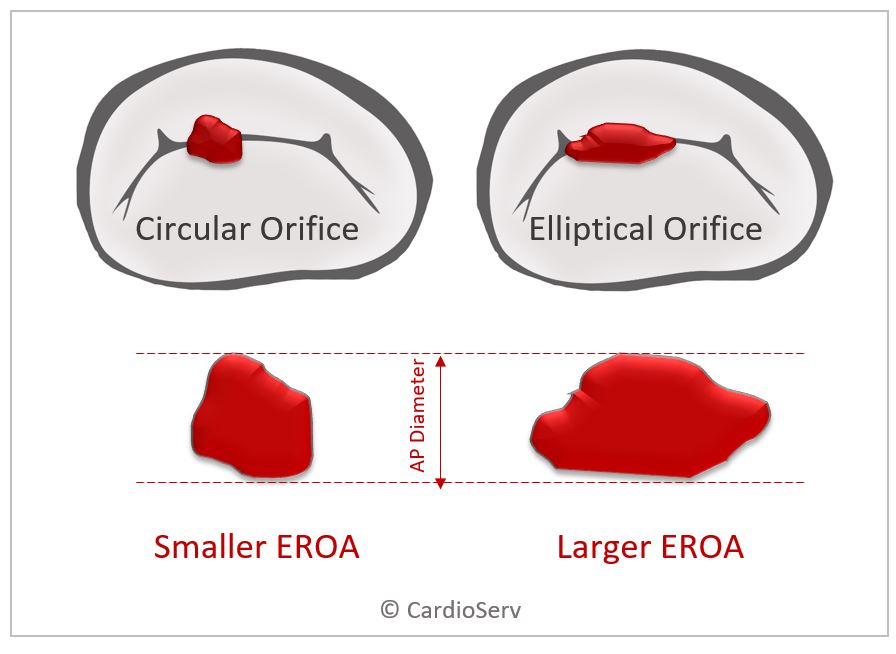
The Vena Contracta is the narrowest portion of the MR jet and in the presence of a circular-shaped MR orifice, the cross-sectional area directly represents the orifice area (EROA) which is a true parameter of MR severity. But…MR orifices are not always circular, they can be elliptical shaped and extend along the MV coaptation line as we see with secondary MR.

Primary MR
- Primary MR orifice is usually circular
- VCW accurately represents the regurgitant orifice area (EROA)
- MR caused by the mitral leaflets – prolapse, flail, etc
Secondary MR
It cannot be stressed enough that secondary MR often presents with an elliptical-shaped MR opening (orifice). This is key to understanding the limitations of VCW in secondary MR.
- Secondary MR orifice is usually elliptical-shaped (slit shaped)
- VCW underestimates MR severity
- MR caused by LV dysfunction, usually ischemic cardiomyopathy
- Mitral valve tethering and annulus dilatation
- MR orifice stretched out and runs along the line of MV coaptation
VENA CONTRACTA AND ORIFICE SHAPE
The VCW is the diameter used to calculate the cross-sectional area (CSA) of the MR orifice. (Remember, CSA = EROA – a true parameter of MR severity).
An elliptical shape can share the same diameter as a circle yet have a much greater area than the circle. You can see how much an elliptical area can be underestimated with the examples below.

HOW THIS RELATES SPECIFICALLY TO VENA CONTRACTA WIDTH (VCW)
The Vena Contracta Width is measured in the parasternal long-axis view. From this plane, only the anterior-posterior (AP) diameter is measured.

If the MR orifice is circular, the AP measurement of the VCW will accurately calculate the cross-sectional area of the vena contracta which represents the effective regurgitant orifice area (EROA).

SECONDARY MR AND VENA CONTRACTA WIDTH (VCW)
However, with secondary MR, the regurgitant orifice is not circular but rather a slit-shaped orifice that runs along the coaptation line. The mathematical circular assumptions no longer hold true. The true shape and size of the orifice cannot be determined by the AP diameter of the vena contracta width.

One solution to this dilemma would be to image the vena contracta in 3D, allowing the visualization and measurement of the true cross-sectional area of the narrowest portion of the MR jet. Unfortunately, we do not always have the time to interrogate the MR vena contracta in 3D.
So now what?!
In the absence of 3D imaging of the vena contracta, it is important to remember that secondary MR is most likely being underestimated. Awareness that the VCW is underestimated allows us to provide an integrated approach to the quantification of MR.
There are many factors that help us make the final diagnosis of MR severity including:
- Vena contracta width
- Proximal flow convergence radius
- PW and CW markers
- PISA and volumetric methods to calculate:
- EROA (Effective Regurgitant Orifice)
- RVol (Regurgitant Volume)
- RF% (regurgitant Fraction)
Our awareness of the limitations of these measures will help us to understand which measure is most likely to be accurate. Remember, the whole picture has to be taken into account (2D, color flow, Doppler, quantification, mechanism, etc.) to correctly diagnose MR severity.
Secondary MR = elliptical orifice = underestimation of MR orifice
5 things you need to know about Secondary MR and Vena Contracta Width (VCW)
- Vena contracta = narrowest area of the MR jet
- The CSA of the vena contracta is a true measure of the regurgitant orifice area (EROA)
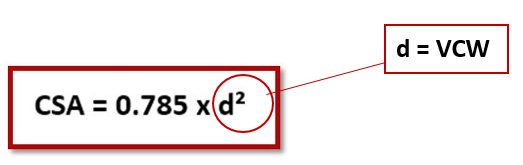
- CSA of MR orifice = 0.785 x d2 (assumes circular shape)
- d = Vena Contracta Width (measured in PLAX – AP measurement)
- MR mechanisms affect MR orifice shape
- Secondary MR often have elliptical orifices
- The PLAX AP measurement of the VCW does not reflect the largest diameter of an elliptical orifice…therefore
- Underestimated Vena Contrata Width = underestimated Cross Sectional Area = Underestimated EROA = underestimated MR severity.

PURCHASE THE 5.0 CAT 1 AMA CME COURSE MASTERING ADVANCED MR QUANTIFICATION.
Judith Buckland, MBA, RDCS, FASE
Reference
ASE GUIDELINES AND STANDARDS. Recommendations for Noninvasive Evaluation of Native Valvular Regurgitation