We recently reviewed a case during a local hospital quality improvement meeting that required us to assess whether or not there was prosthetic aortic valve stenosis. It was interesting to touch up on the key parameters that should be assessed. This week we will review the key points for imaging and interpreting prosthetic aortic valve stenosis with echocardiography.
Imaging the heart status post valve repair can be challenging, especially due to the artifact caused by some prosthetic valves. This is why we encourage off axis imaging whenever necessary to better visualize your region of interest. Pay attention to the following items during an echocardiogram of a prosthetic valve:
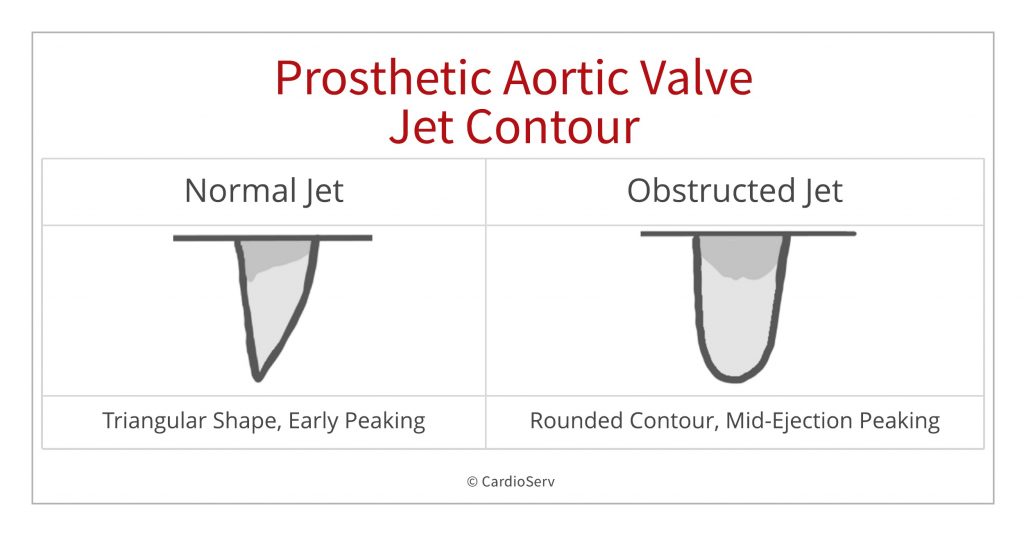
The jet contour can provide us with valuable information. Although not quantitative it is a qualitative measure and is considered a valuable index of prosthetic valve function
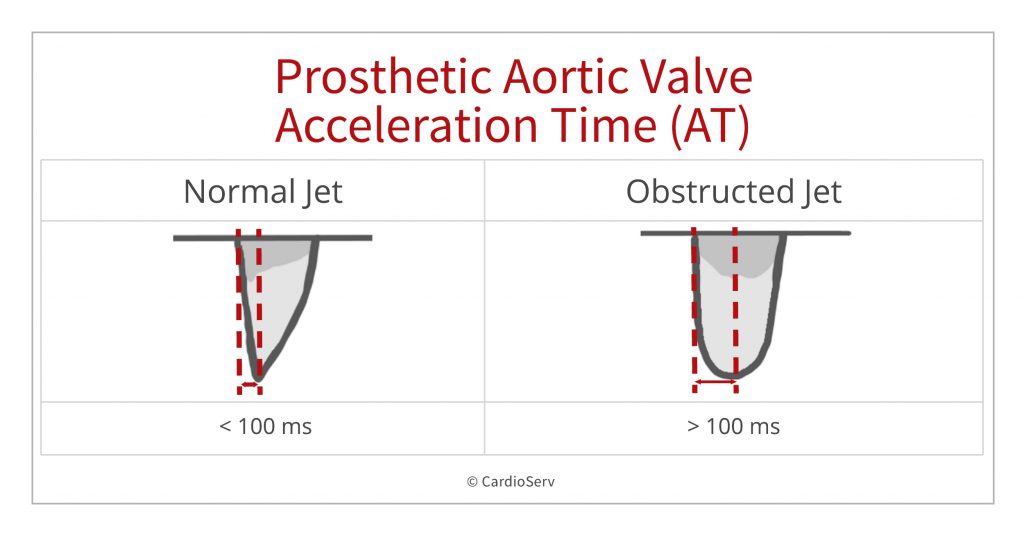
While the jet contour is qualitative we can use the acceleration time as a quantitative measure to assess prosthetic aortic valve stenosis. An acceleration time > 100 m/s differentiates between normal and stenotic prosthetic valves.
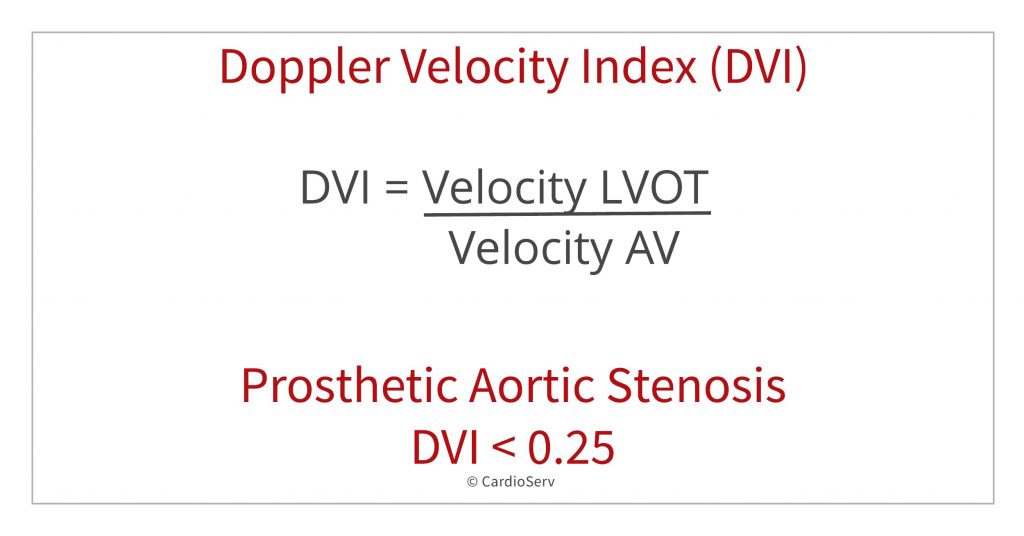
DVI – Doppler Velocity Index
Another quantitative measurement is the Doppler Velocity Index (DVI). The DVI is a dimensionless index that is great to use in the presence of prosthetic valves because the value is not flow dependent and is less dependent on valve size. It’s especially useful when the valve size is unknown. DVI < 0.25 is highly suggestive of significant valve obstruction
How to obtain the DVI
DVI = VelocityLVOT / VelocityPrAV
DVI < 0.25 is highly suggestive of significant valve obstruction
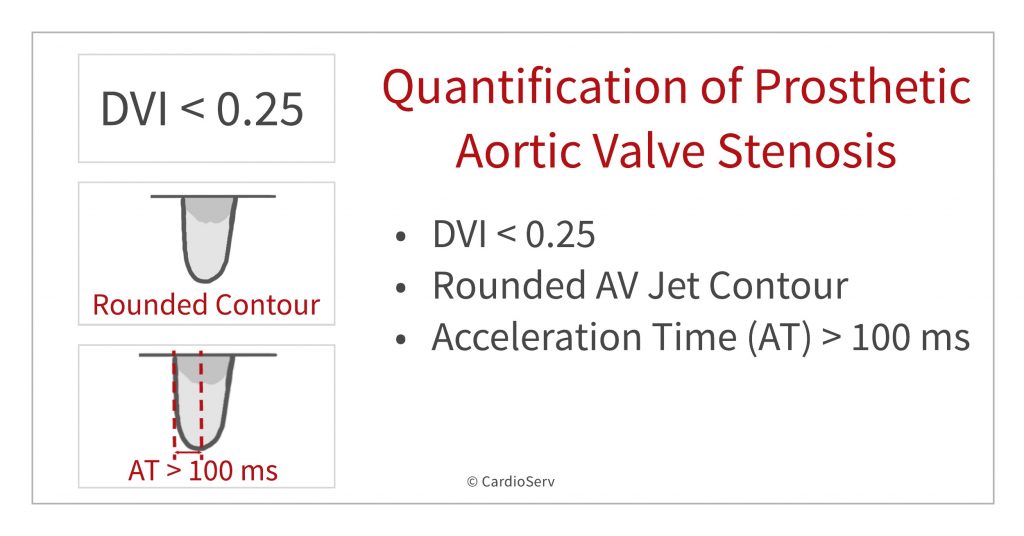
When quantifying prosthetic aortic valve stenosis on echocardiography we learned that three parameters can help us determine prosthetic aortic valve stenosis:
Zoghbi, et al. Evaluation of Prosthetic Valves With Echocardiography and Doppler Ultrasound. American Society of Echocardiography. 2009. Retrieved from: https://www.asecho.org/wp-content/uploads/2014/05/2009_Evaluation-of-Prosthetic-Valves.pdf

Judith Buckland, MBA, RDCS, FASE









Jun
2019
Jun
2019
Jun
2019
Jul
2019
Jul
2019
Jul
2019
Aug
2019
Nov
2019
Dec
2019
Feb
2020